Cecchetto Giovanni
Department of Women's and Children's Health, Pediatric Surgery Unit, University Hospital of Padua, Padua, Italy.
J Indian Assoc Pediatr Surg. 2014 Oct;19(4):189-94. doi: 10.4103/0971-9261.141995.
PEDIATRIC GERM CELL TUMORS (GCT) ARE RARE TUMORS: 80% are benign, 20% malignant (2-3% of all malignant pediatric tumors). The gonadal sites (ovary and testis) account for 40% of cases.
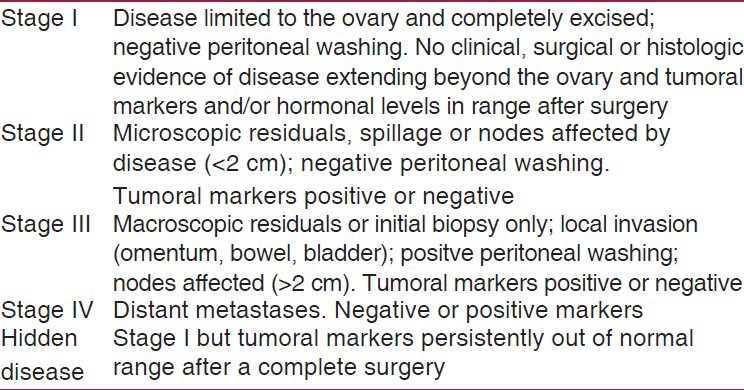
Represent 30% of GCTs and 70% of neoplastic ovarian masses, being the most common ovarian neoplasms in children and teenagers. Benign and immature forms (teratomas) constitute about 80% of all ovarian GCTs, malignant forms represent 20% increasing during adolescence. The most common malignant entity in children is the yolk sac tumors (YST); dysgerminoma is frequent during adolescence and being bilateral in 10% of cases. Presentation is similar in malignant and benign lesions; abdominal pain (70-80%) and lower abdominal mass are common symptoms. Evaluation of alpha-fetoprotein (αFP) or beta subunit of human chorionic gonadotropin (βHCG) is essential to address the nature of the tumors: Their elevation means presence of malignancy. Surgery includes intraoperative staging procedures and requires ovariectomy or ovarosalpingectomy for malignant lesions, but may be conservative in selected benign tumors. Since malignant GCTs are very chemosensitive, primary chemotherapy is recommended in metastatic or locally advanced tumors.
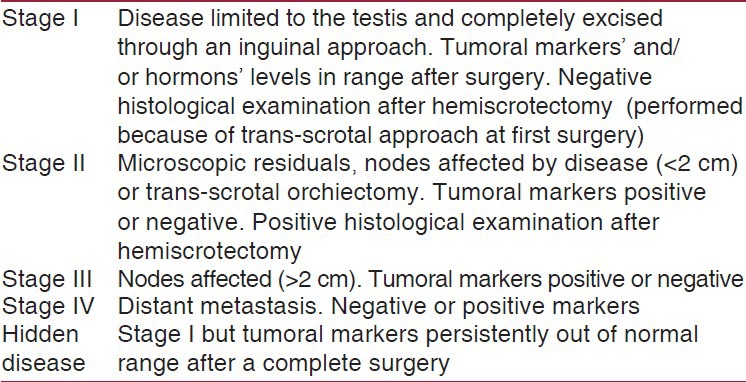
Represent 10% of pediatric GCT, and about 30% of malignant GCT with two age peaks: Children <3 years may experience mature teratoma and malignant GCTs, represented almost exclusively by YST, while adolescents may also show seminomas or other mixed tumors. The main clinical feature is a painless scrotal mass. Surgery represents the cornerstone of the management of testicular GCTs, with an inguinal approach and a primary high orchidectomy for malignant tumors, while a testis-sparing surgery can be considered for benign lesions. A retroperitoneal lymph node (LN) biopsy may be necessary to define the staging when the involvement of retroperitoneal LN is uncertain at imaging investigations.
Patients with gonadal malignant GCTs fare better than those with extragonadal mediastinal germ cell tumors (MGCTs) and survival rate exceeds 90% in localized forms. Chemotherapy has significantly improved the outcome of malignant forms since the introduction of platinum based regimens. The surgical procedure has to be performed in agreement with the ongoing protocols.
小儿生殖细胞肿瘤(GCT)较为罕见:80%为良性,20%为恶性(占所有小儿恶性肿瘤的2 - 3%)。性腺部位(卵巢和睾丸)占病例的40%。
卵巢GCT:占GCT的30%,占卵巢肿瘤性肿块的70%,是儿童和青少年中最常见的卵巢肿瘤。良性和不成熟型(畸胎瘤)约占所有卵巢GCT的80%,恶性型占20%,在青春期有所增加。儿童中最常见的恶性类型是卵黄囊瘤(YST);无性细胞瘤在青春期较为常见,10%的病例为双侧性。恶性和良性病变的表现相似;腹痛(70 - 80%)和下腹部肿块是常见症状。评估甲胎蛋白(αFP)或人绒毛膜促性腺激素β亚基(βHCG)对于明确肿瘤性质至关重要:其升高意味着存在恶性肿瘤。手术包括术中分期程序,恶性病变需行卵巢切除术或卵巢输卵管切除术,但对于某些良性肿瘤可能采取保守手术。由于恶性GCT对化疗非常敏感,对于转移性或局部晚期肿瘤建议进行一线化疗。
睾丸GCT:占小儿GCT的10%,约占恶性GCT的30%,有两个年龄高峰:3岁以下儿童可能出现成熟畸胎瘤和恶性GCT,几乎仅由YST代表,而青少年也可能出现精原细胞瘤或其他混合性肿瘤。主要临床特征是无痛性阴囊肿块。手术是睾丸GCT治疗的基石,恶性肿瘤采用腹股沟入路和一期高位睾丸切除术,而良性病变可考虑保留睾丸手术。当影像学检查不确定腹膜后淋巴结是否受累时,可能需要进行腹膜后淋巴结活检以明确分期。
性腺恶性GCT患者的预后优于性腺外纵隔生殖细胞肿瘤(MGCT)患者,局限性病例的生存率超过90%。自引入铂类方案以来,化疗显著改善了恶性病例的预后。手术程序必须按照现行方案进行。