Steel N, Hardcastle A C, Bachmann M O, Richards S H, Mounce L T A, Clark A, Lang I, Melzer D, Campbell J
Department of Population Health and Primary Care, Norwich Medical School, University of East Anglia, Norwich, UK.
University of Exeter Medical School, Exeter, UK.
BMJ Open. 2014 Oct 24;4(10):e005530. doi: 10.1136/bmjopen-2014-005530.
We compared the distribution by wealth of self-reported illness burden (estimated from validated scales, biomarker and reported symptoms) for angina, cataract, depression, diabetes and osteoarthritis, with the distribution of self-reported medical diagnosis and treatment. We aimed to determine if the greater illness burden borne by poorer participants was matched by appropriately higher levels of diagnosis and treatment.
The English Longitudinal Study of Ageing, a panel study of 12,765 participants aged 50 years and older in four waves from 2004 to 2011, selected using a stratified random sample of households in England. Distribution of illness burden, diagnosis and treatment by wealth was estimated using regression analysis.
The main outcome measures were ORs for the illness burden, diagnosis and treatment, respectively, adjusted for age, sex and wealth. We estimated the illness burden for angina with the Rose Angina scale, diabetes with fasting glycosylated haemoglobin, depression with the Centre for Epidemiologic Studies Depression Scale, osteoarthritis with self-reported pain and disability and cataract with self-reported poor vision. Medical diagnoses were self-reported for all conditions. Treatment was defined as β-blocker prescription for angina, surgery for osteoarthritis and cataract, and receipt of predefined effective interventions for diabetes and depression.
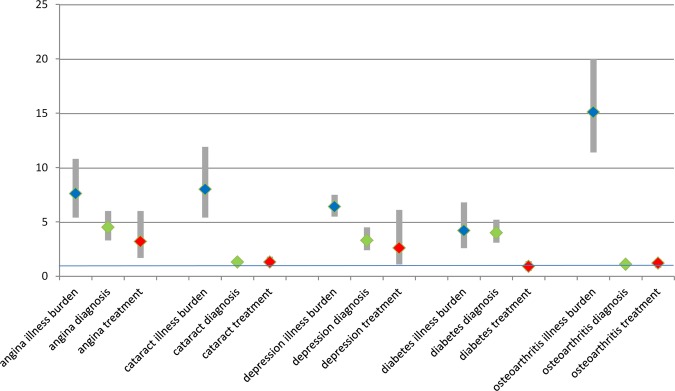
Compared with the wealthiest, the least wealthy participant had substantially higher odds for illness burden from any of the five conditions at all four time points, with ORs ranging from 4.2 (95% CI 2.6 to 6.8) for diabetes to 15.1 (11.4 to 20.0) for osteoarthritis. The ORs for diagnosis and treatment were smaller in all five conditions, and ranged from 0.9 (0.5 to 1.4) for diabetes treatment to 4.5 (3.3 to 6.0) for angina diagnosis.
The substantially higher illness burden in less wealthy participants was not matched by appropriately higher levels of diagnosis and treatment.
我们比较了心绞痛、白内障、抑郁症、糖尿病和骨关节炎自我报告的疾病负担(根据经过验证的量表、生物标志物和报告的症状估算)按财富水平的分布情况,以及自我报告的医疗诊断和治疗情况。我们旨在确定较贫困参与者所承担的更高疾病负担是否与相应更高水平的诊断和治疗相匹配。
英国老龄化纵向研究,这是一项针对12765名年龄在50岁及以上参与者的队列研究,于2004年至2011年分四波进行,采用英格兰家庭分层随机抽样选取。通过回归分析估算疾病负担、诊断和治疗按财富水平的分布情况。
主要结局指标分别为疾病负担、诊断和治疗的比值比(OR),并对年龄、性别和财富进行了调整。我们使用罗斯心绞痛量表估算心绞痛的疾病负担,使用空腹糖化血红蛋白估算糖尿病的疾病负担,使用流行病学研究中心抑郁量表估算抑郁症的疾病负担,使用自我报告的疼痛和残疾情况估算骨关节炎的疾病负担,使用自我报告的视力不佳情况估算白内障的疾病负担。所有疾病的医疗诊断均为自我报告。治疗定义为心绞痛使用β受体阻滞剂处方、骨关节炎和白内障进行手术,以及糖尿病和抑郁症接受预先定义的有效干预措施。
与最富有的人相比,最贫穷的参与者在所有四个时间点上,患这五种疾病中任何一种的疾病负担几率都显著更高,糖尿病的OR值范围为4.2(95%CI 2.6至6.8),骨关节炎的OR值范围为15.1(11.4至20.0)。在所有五种疾病中,诊断和治疗的OR值较小,糖尿病治疗的OR值范围为0.9(0.5至1.4),心绞痛诊断的OR值范围为4.5(3.3至6.0)。
较贫困参与者更高的疾病负担并未与相应更高水平的诊断和治疗相匹配。