Richardson-Harman Nicola, Hendrix Craig W, Bumpus Namandjé N, Mauck Christine, Cranston Ross D, Yang Kuo, Elliott Julie, Tanner Karen, McGowan Ian, Kashuba Angela, Anton Peter A
Alpha StatConsult, LLC, Damascus, MD, United States of America.
Departments of Medicine and Pharmacology, Johns Hopkins University School of Medicine, Baltimore, MD, United States of America.
PLoS One. 2014 Oct 28;9(10):e111507. doi: 10.1371/journal.pone.0111507. eCollection 2014.
This study was designed to assess the dose-response relationship between tissue, blood, vaginal and rectal compartment concentrations of tenofovir (TFV) and tenofovir diphosphate (TFVdp) and ex vivo rectal HIV suppression following oral tenofovir disoproxil fumarate (TDF) and rectal administration of TFV 1% vaginally-formulated gel.
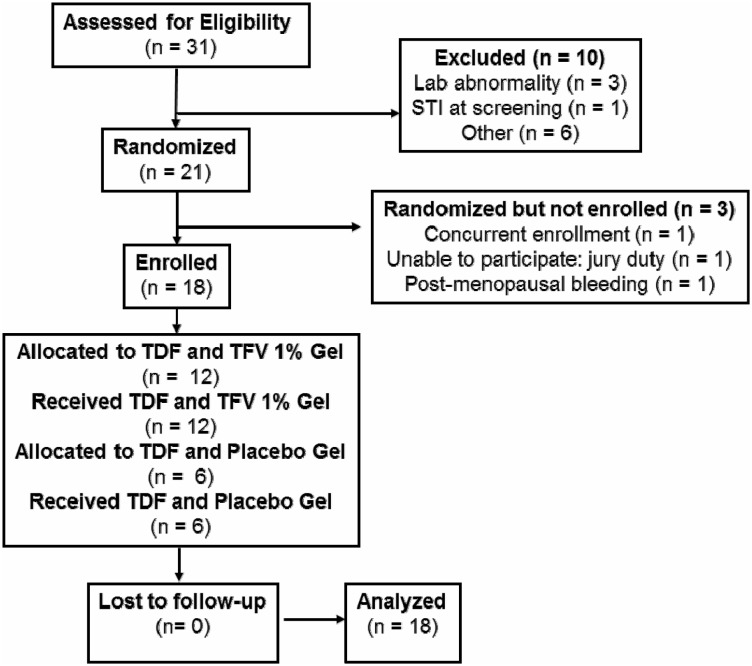
Phase 1, randomized, two-site (US), double-blind, placebo-controlled study of sexually-abstinent males and females.
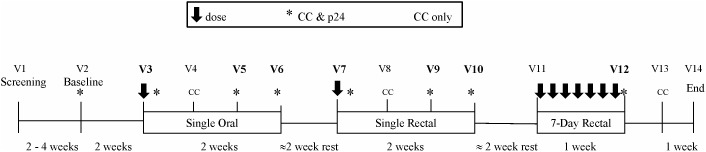
Eighteen participants received a single 300 mg exposure of oral TDF and were then randomized 2∶1 to receive a single then seven-daily rectal exposures of TFV 1% gel (40 mg TFV per 4 ml gel application) or hydroxyethyl-cellulose (HEC) placebo gel. Blood and rectal biopsies were collected for pharmacokinetic TDF and TFVdp analyses and ex vivo HIV-1 challenge.
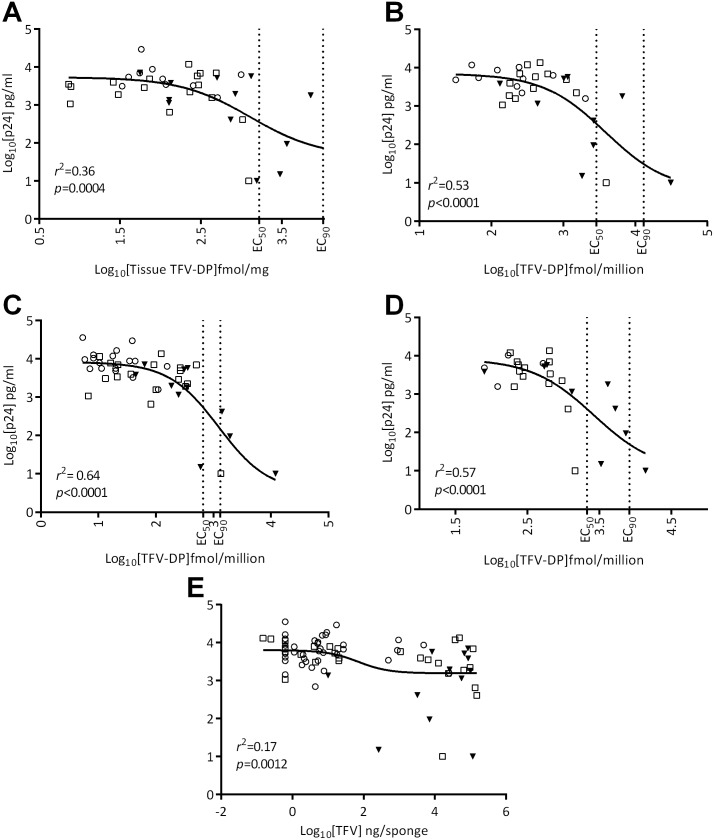
There was a significant fit for the TFVdp dose-response model for rectal tissue (p = 0.0004), CD4+MMC (p<0.0001), CD4-MMC (p<0.0001), and TotalMMC (p<0.0001) compartments with r2 ranging 0.36-0.64. Higher concentrations of TFVdp corresponded with lower p24, consistent with drug-mediated virus suppression. The single oral treatment failed to provide adequate compartment drug exposure to reach the EC50 of rectal tissue TFVdp predicted to be necessary to suppress HIV in rectal tissue. The EC50 for CD4+MMC was within the single topical treatment range, providing evidence that a 1% topical, vaginally-formulated TFV gel provided in-vivo doses predicted to provide for 50% efficacy in the ex vivo assay. The 7-daily topical TFV gel treatment provided TFVdp concentrations that reached EC90 biopsy efficacy for CD4-MMC, CD4+MMC and TotalMMC compartments.
The TFVdp MMC compartment (CD4+, CD4- and Total) provided the best surrogate for biopsy infectibility and the 7-daily topical TFV gel treatment provided the strongest PK profile for HIV suppression. ClinicalTrials.gov NCT00984971.
本研究旨在评估口服替诺福韦酯富马酸盐(TDF)及经直肠给予1%阴道用替诺福韦(TFV)凝胶后,替诺福韦(TFV)和替诺福韦二磷酸酯(TFVdp)在组织、血液、阴道及直肠腔室中的浓度与离体直肠HIV抑制之间的剂量反应关系。
一项针对禁欲的男性和女性的1期、随机、双中心(美国)、双盲、安慰剂对照研究。
18名参与者接受单次300mg口服TDF暴露,然后按2∶1随机分组,分别接受单次及随后连续7天的直肠给予1% TFV凝胶(每4ml凝胶含40mg TFV)或羟乙基纤维素(HEC)安慰剂凝胶。采集血液和直肠活检样本用于药代动力学TDF和TFVdp分析以及离体HIV-1挑战。
直肠组织(p = 0.0004)、CD4+MMC(p<0.0001)、CD4-MMC(p<0.0001)和TotalMMC(p<0.0001)腔室的TFVdp剂量反应模型拟合良好,r2范围为0.36 - 0.64。TFVdp浓度越高,p24越低,这与药物介导的病毒抑制一致。单次口服治疗未能提供足够的腔室药物暴露以达到预测的直肠组织中抑制HIV所需的直肠组织TFVdp的EC50。CD4+MMC的EC50在单次局部治疗范围内,这表明1%局部阴道用TFV凝胶提供的体内剂量预计在离体试验中具有50%的疗效。连续7天局部给予TFV凝胶治疗使TFVdp浓度达到了CD4-MMC、CD4+MMC和TotalMMC腔室活检EC90疗效。
TFVdp MMC腔室(CD4+、CD4-和Total)为活检感染性提供了最佳替代指标,连续7天局部给予TFV凝胶治疗为HIV抑制提供了最强的药代动力学特征。ClinicalTrials.gov NCT00984971。