Hofstra Laura Marije, Mudrikova Tania, Stam Arjen J, Otto Sigrid, Tesselaar Kiki, Nijhuis Monique, Wensing Annemarie M J
Department of Medical Microbiology, Virology, University Medical Center Utrecht, Utrecht, the Netherlands.
Department of Internal Medicine and Infectious Diseases, University Medical Center Utrecht, Utrecht, the Netherlands.
PLoS One. 2014 Oct 29;9(10):e110749. doi: 10.1371/journal.pone.0110749. eCollection 2014.
It has been suggested that low-level viremia or blips in HIV-infected patients on antiretroviral treatment are related to assay variation and/or increased sensitivity of new commercial assays. The 50-copy cut-off for virologic failure is, therefore, under debate.
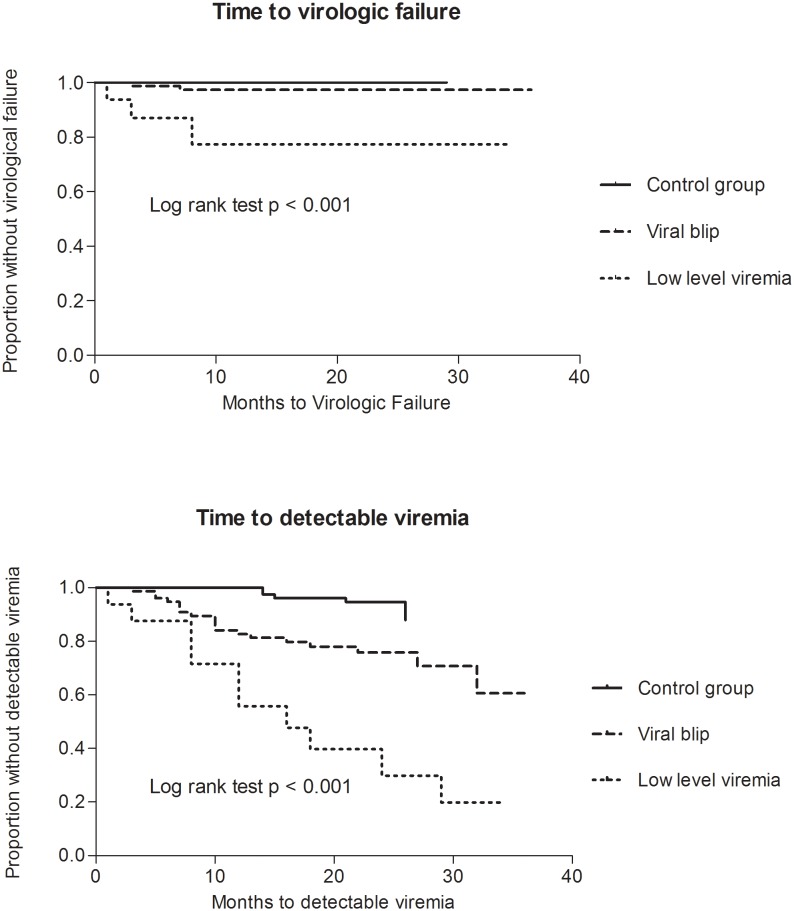
Treated patients with low-level viremia (persistent viral loads (VL) of 50-1000 copies/mL, group A, N = 16) or a blip (single detectable VL, group B, N = 77) were compared to a control group (consistently suppressed viremia since start therapy (<50 copies/mL), N = 79). Residual viremia (detectable viral RNA <50 copies/ml) in the year preceding the first VL above 50 copies/mL (T0) was determined using Roche Cobas-Amplicor v1.5 or CAP-CTM v2.0. Subsequent virologic failure (2 consecutive VLs>500 or 1 VL>1000 copies/mL that was not followed by a VL<50 copies/mL; median follow up 34 months) was assessed.
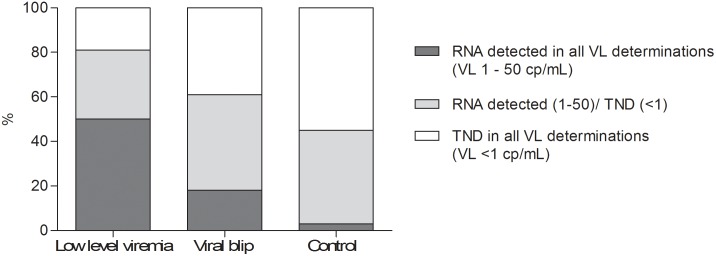
Significantly more patients in groups A and B had residual viremia in the year preceding T0 compared to controls (50% and 19% vs 3% respectively; p<0.001). Residual viremia was associated with development of low-level viremia or blips (OR 10.9 (95% CI 2.9-40.6)). Subsequent virologic failure was seen more often in group A (3/16) and B (2/77) than in the control group (0/79).
Residual viremia is associated with development of blips and low-level viremia. Virologic failure occurred more often in patients with low-level viremia. These results suggest that low-level viremia results from viral production/replication rather than only assay variation.
有观点认为,接受抗逆转录病毒治疗的HIV感染患者出现的低水平病毒血症或病毒载量波动与检测方法的差异和/或新型商业检测方法敏感性的提高有关。因此,病毒学失败的50拷贝临界值存在争议。
将出现低水平病毒血症(持续病毒载量(VL)为50 - 1000拷贝/毫升,A组,N = 16)或病毒载量波动(单次可检测到的VL,B组,N = 77)的接受治疗患者与对照组(自开始治疗以来病毒血症持续被抑制(<50拷贝/毫升),N = 79)进行比较。使用罗氏Cobas - Amplicor v1.5或CAP - CTM v2.0测定首次VL高于50拷贝/毫升(T0)前一年的残余病毒血症(可检测到的病毒RNA<50拷贝/毫升)。评估随后的病毒学失败情况(连续两次VL>500或一次VL>1000拷贝/毫升且随后未出现VL<50拷贝/毫升;中位随访34个月)。
与对照组相比,A组和B组在T0前一年有残余病毒血症的患者显著更多(分别为50%和19%,而对照组为3%;p<0.001)。残余病毒血症与低水平病毒血症或病毒载量波动的发生相关(比值比10.9(95%置信区间2.9 - 40.6))。A组(3/16)和B组(2/77)随后出现病毒学失败的情况比对照组(0/79)更常见。
残余病毒血症与病毒载量波动和低水平病毒血症的发生相关。低水平病毒血症患者更常出现病毒学失败。这些结果表明,低水平病毒血症是由病毒产生/复制引起的,而非仅仅是检测方法的差异。