Kennedy William P, Simon J Abraham, Offutt Carolyn, Horn Priscilla, Herman Ann, Townsend Michael J, Tang Meina T, Grogan Jane L, Hsieh Frank, Davis John C
Arthritis Res Ther. 2014 Oct 30;16(5):467. doi: 10.1186/s13075-014-0467-3.
Tumor necrosis factor (TNF) and, possibly, lymphotoxin alpha (LTα) signaling contribute to inflammation and rheumatoid arthritis (RA) pathogenesis. Pateclizumab (anti-lymphotoxin- alpha; MLTA3698A) is a humanized monoclonal antibody that blocks and depletes anti-LTα. This phase 2, randomized, head-to-head, active- and placebo-controlled trial examined the safety and efficacy of pateclizumab compared to adalimumab in RA patients with an inadequate response to disease-modifying antirheumatic drugs (DMARD-IR).
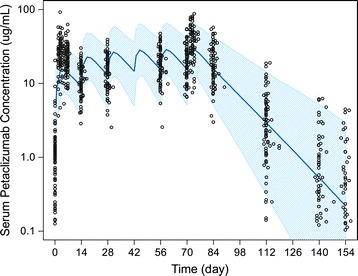
Patients (n = 214) with active RA (≥ 6 swollen and tender joints, C-reactive protein ≥ 10 mg/L) on oral DMARDs were randomized (2:2:1) to receive pateclizumab 360 mg, adalimumab 40 mg, or placebo subcutaneously every 2 weeks. The primary endpoint, 4-variable, 28-joint disease activity score erythrocyte sedimentation rate (DAS28(4)-ESR) response, was evaluated at 12 weeks using an analysis of covariance (ANCOVA) model with adjustments for concomitant DMARD use and geographic region. Secondary efficacy endpoints included American College of Rheumatology (ACR) 20, ACR50, and ACR70 responses at Day 85. Pharmacokinetics, pharmacodynamics, and immunogenicity of pateclizumab were assessed.
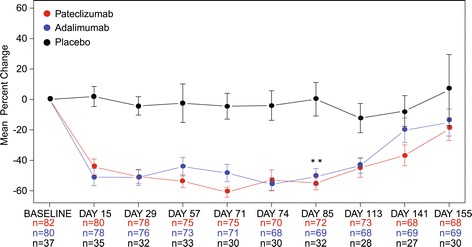
Pateclizumab reduced the DAS28(4)-ESR response (-1.89) at 12 weeks, however, this did not reach statistical significance compared to placebo (-1.54), while adalimumab (-2.52) differed significantly from both placebo and pateclizumab. Pateclizumab 12-week ACR20, ACR50 and ACR70 response rates (64%, 33%, and 14%) suggested clinical activity but were not statistically significant compared to placebo rates (46%, 24%, and 8%, respectively). CXCL13 serum levels decreased significantly following pateclizumab and adalimumab administration, demonstrating pharmacological target engagement by both drugs. Overall, adverse events (AEs) were comparable among all cohorts. Infections were the most common AE, occurring with comparable frequency in all groups. Serious AEs occurred in 0% of pateclizumab, 5.9% of adalimumab, and 2.3% of placebo patients, with serious infection in 2.3% of adalimumab patients and none in pateclizumab and placebo patients.
Pateclizumab had a good safety profile in patients inadequately responsive to DMARDs, but no statistically significant improvement in RA signs and symptoms after 12 weeks of treatment. Adalimumab demonstrated efficacy and safety comparable to published results in this head-to-head comparison in DMARD-IR RA patients.
ClinicalTrials.gov NCT01225393, Registered 18 October 2010.
肿瘤坏死因子(TNF)以及可能的淋巴毒素α(LTα)信号传导参与炎症和类风湿性关节炎(RA)的发病机制。帕泰利珠单抗(抗淋巴毒素α;MLTA3698A)是一种人源化单克隆抗体,可阻断并消耗抗LTα。这项2期随机、头对头、活性药物和安慰剂对照试验,比较了帕泰利珠单抗与阿达木单抗在对改善病情抗风湿药物(DMARD)反应不足的RA患者中的安全性和疗效。
口服DMARDs且患有活动性RA(≥6个肿胀和压痛关节,C反应蛋白≥10mg/L)的患者(n = 214)被随机分组(2:2:1),每2周皮下注射360mg帕泰利珠单抗、40mg阿达木单抗或安慰剂。主要终点为4变量28关节疾病活动评分红细胞沉降率(DAS28(4)-ESR)反应,在第12周时使用协方差分析(ANCOVA)模型进行评估,并对同时使用的DMARD和地理区域进行调整。次要疗效终点包括第85天时美国风湿病学会(ACR)20、ACR50和ACR70反应。评估了帕泰利珠单抗的药代动力学、药效学和免疫原性。
帕泰利珠单抗在第12周时降低了DAS28(4)-ESR反应(-1.89),然而,与安慰剂(-1.54)相比,这未达到统计学显著性,而阿达木单抗(-2.52)与安慰剂和帕泰利珠单抗均有显著差异。帕泰利珠单抗第12周时的ACR20、ACR50和ACR70反应率(分别为64%、33%和14%)显示出临床活性,但与安慰剂率(分别为46%、24%和8%)相比无统计学显著性。帕泰利珠单抗和阿达木单抗给药后CXCL13血清水平显著下降,表明两种药物均作用于药理学靶点。总体而言,所有队列中的不良事件(AE)相当。感染是最常见的AE,在所有组中发生频率相当。严重AE在帕泰利珠单抗组中的发生率为0%,阿达木单抗组为5.9%,安慰剂组为2.3%,阿达木单抗组中2.3.3%的患者发生严重感染,帕泰利珠单抗组和安慰剂组均无。
帕泰利珠单抗在对DMARD反应不足的患者中具有良好的安全性,但治疗12周后RA体征和症状无统计学显著改善。在这项针对DMARD反应不足的RA患者的头对头比较中,阿达木单抗显示出与已发表结果相当的疗效和安全性。
ClinicalTrials.gov NCT01225393,于2010年10月18日注册。