Ernstbrunner Matthäus, Kostner Lisa, Kimberger Oliver, Wabel Peter, Säemann Marcus, Markstaller Klaus, Fleischmann Edith, Kabon Barbara, Hecking Manfred
Medical University of Vienna, Department of Anaesthesiology and Critical Care Medicine, Vienna, Austria.
Fresenius Medical Care, Bad Homburg, Germany.
PLoS One. 2014 Oct 31;9(10):e111139. doi: 10.1371/journal.pone.0111139. eCollection 2014.
Technically assisted assessment of volume status before surgery may be useful to direct intraoperative fluid administration. We therefore tested a recently developed whole-body bioimpedance spectroscopy device to determine pre- to postoperative fluid distribution.
Using a three-compartment physiologic tissue model, the body composition monitor (BCM, Fresenius Medical Care, Germany) measures total body fluid volume, extracellular volume, intracellular volume and fluid overload as surplus or deficit of 'normal' extracellular volume. BCM-measurements were performed before and after standardized general anaesthesia for gynaecological procedures (laparotomies, laparoscopies and vaginal surgeries). BCM results were blinded to the attending anaesthesiologist and data analysed using the 2-sided, paired Student's t-test and multiple linear regression.
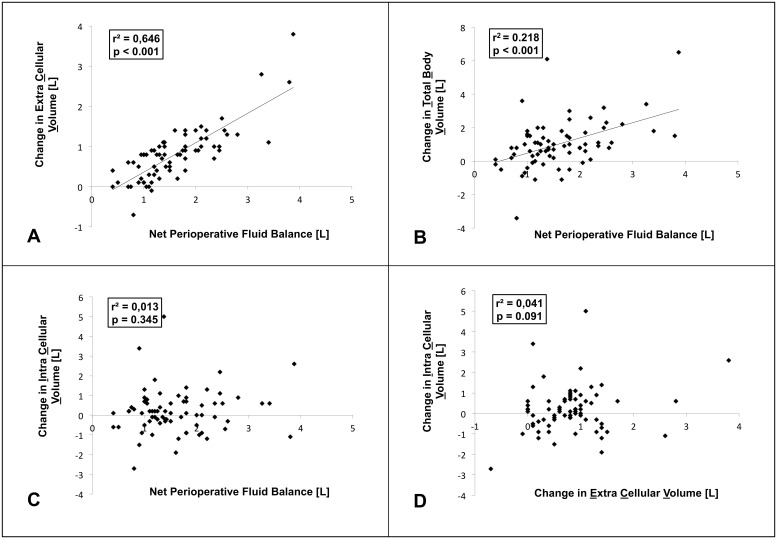
In 71 females aged 45 ± 15 years with body weight 67 ± 13 kg and Duration of anesthesia 154 ± 69 minutes [corrected] duration of anaesthesia 154 ± 68 min, pre- to postoperative fluid overload increased from -0.7 ± 1.1 L to 0.1 ± 1.0 L, corresponding to -5.1 ± 7.5% and 0.8 ± 6.7% of normal extracellular volume, respectively (both p<0.001), after patients had received 1.9 ± 0.9 L intravenous crystalloid fluid. Perioperative urinary excretion was 0.3 ± 0.2 L [corrected]. The increase in extracellular volume was paralleled by an increase in total body fluid volume, while intracellular volume increased only slightly and without reaching statistical significance (p = 0.15). Net perioperative fluid balance (administered fluid volume minus urinary excretion) was significantly associated with change in extracellular volume (r(2) = 0.65), but was not associated with change in intracellular volume (r(2) = 0.01).
Routine intraoperative fluid administration results in a significant, and clinically meaningful increase in the extracellular compartment. BCM-measurements yielded plausible results and may become useful to guide intraoperative fluid therapy in future studies.
术前通过技术手段辅助评估容量状态可能有助于指导术中液体输注。因此,我们测试了一种最近研发的全身生物电阻抗光谱设备,以确定术前至术后的液体分布情况。
使用三室生理组织模型,人体成分监测仪(BCM,德国费森尤斯医疗集团)可测量总体液量、细胞外液量、细胞内液量以及作为“正常”细胞外液量盈余或不足的液体超负荷情况。在妇科手术(剖腹手术、腹腔镜手术和阴道手术)的标准化全身麻醉前后进行BCM测量。BCM结果对主治麻醉医生保密,并使用双侧配对学生t检验和多元线性回归分析数据。
71名年龄45±15岁、体重67±13 kg且麻醉持续时间为154±69分钟[校正后麻醉持续时间为154±68分钟]的女性患者,在接受1.9±0.9 L静脉晶体液后,术前至术后的液体超负荷从-0.7±1.1 L增加至0.1±1.0 L,分别相当于正常细胞外液量的-5.1±7.5%和0.8±6.7%(均p<0.001)。围手术期尿量为0.3±0.2 L[校正后]。细胞外液量增加的同时总体液量也增加,而细胞内液量仅略有增加且未达到统计学意义(p = 0.15)。围手术期净液体平衡(输注液体量减去尿量)与细胞外液量变化显著相关(r(2) = 0.65),但与细胞内液量变化无关(r(2) = 0.01)。
常规术中液体输注导致细胞外液显著且具有临床意义的增加。BCM测量结果合理,可能在未来研究中有助于指导术中液体治疗。