Tittle Victoria, Cenderello Giovanni, Pasa Ambra, Patel Preya, Artioli Stefania, Dentone Chiara, Fraccaro Paolo, Giacomini Mauro, Setti Maurizio, Di Biagio Antonio, Nelson Mark
HIV Unit, Chelsea and Westminster Hospital, London, UK.
Infectious Diseases Unit, EO Ospedali Galliera, Genoa, Italy.
J Int AIDS Soc. 2014 Nov 2;17(4 Suppl 3):19712. doi: 10.7448/IAS.17.4.19712. eCollection 2014.
This study compares the trends of HIV inpatient admissions between a London tertiary HIV centre (United Kingdom) and four infectious disease wards in Italy (IT) to recognize common patterns across Europe.
Data regarding HIV inpatient admissions was collected by using discharge diagnostic codes from 1 January to 31 December 2012, including patient demographics, combined antiretroviral therapy (cART) history, CD4, viral load (VL) and mortality rates. Discharge diagnoses were categorized according to the International Classification of Disease (ICD) 9 and 10 system. All ICD categories that reach a 3% threshold of total admissions were analyzed.
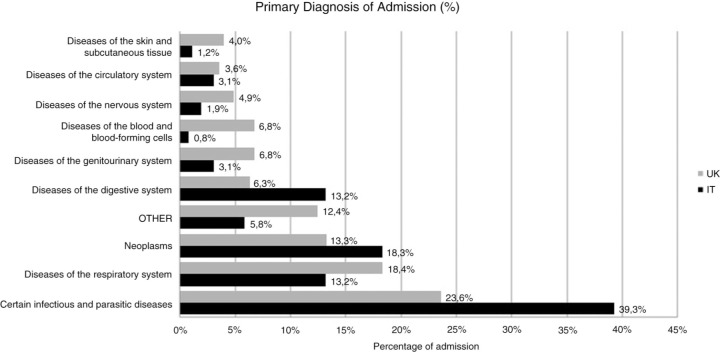
A total of 731 admissions (257 in Italy and 474 in the United Kingdom) for 521 patients (1.5 mean admission per patient). Female admissions were higher in Italy at 22.6% (n=58) compared to 14.9% (n=47) in the United Kingdom. Median age of patients was 47 years old. There was an undetectable VL in 65.8% (n=169) of admissions in Italy and 67.1% (n=319) in the United Kingdom (p=0.385); 86.4% (n=222) and 82.4% (n=389) of admissions were on cART, respectively. Mean CD4 was 302 in Italy compared to 368 in the United Kingdom (p=0.003). Average length of admission was 16 days with a 10.2% (n=21) mortality rate in Italy compared to 8 days with 2.8% (n=9) mortality in the United Kingdom (p<0.001). HCV co-infection was present in 64.6% (n=166) in Italy and 13.5% (n=64) in the United Kingdom and commonest mode of transmission was needle use in Italy (67.3%, n=173) and men who have sex with men in the UK cohort (59.9%, n=284). The cause of inpatient admissions according to ICD codes can be seen in following Figure 1.
Significant differences in the duration of inpatient admission and mortality rates can be observed between these two cohorts which is secondary to the impact of Hepatitis C co-infection in Italy. However increases in the number of Hepatitis C co-infection patients amongst MSM in London has been reported [1] and route of transmission in Italy is shifting towards MSM [2], therefore it is important to learn how HIV is developing and managed in a global context to help plan future for services. The UK cohort demonstrates a wider range of conditions necessitating admission, and with an ageing HIV population, this is expected to increase in the future, requiring general and specialist HIV physicians to work closely together. The HIV-RNA threshold is 400 copies/mL to account for blips according to British HIV Association (BHIVA) Guidelines 2012 [3].
本研究比较了伦敦一家三级艾滋病中心(英国)与意大利四个传染病病房(意大利)的艾滋病住院患者趋势,以识别欧洲各地的常见模式。
通过使用2012年1月1日至12月31日的出院诊断代码收集艾滋病住院患者数据,包括患者人口统计学、联合抗逆转录病毒疗法(cART)史、CD4、病毒载量(VL)和死亡率。出院诊断根据国际疾病分类(ICD)9和10系统进行分类。分析了所有占总入院人数3%阈值的ICD类别。
共731例入院(意大利257例,英国474例),涉及521名患者(平均每人入院1.5次)。意大利女性入院率为22.6%(n = 58),高于英国的14.9%(n = 47)。患者中位年龄为47岁。意大利65.8%(n = 169)的入院患者病毒载量不可检测,英国为67.1%(n = 319)(p = 0.385);分别有86.4%(n = 222)和82.4%(n = 389)的入院患者接受cART治疗。意大利的平均CD4为302,而英国为368(p = 0.003)。意大利的平均住院时间为16天,死亡率为10.2%(n = 21),而英国平均住院时间为8天,死亡率为2.8%(n = 9)(p < 0.001)。意大利64.6%(n = 166)的患者合并丙型肝炎病毒感染,英国为13.5%(n = 64),意大利最常见的传播方式是使用针头(67.3%,n = 173),而英国队列中是男男性行为者(59.9%,n = 284)。根据ICD代码的住院原因见图1。
这两个队列在住院时间和死亡率方面存在显著差异,这是意大利丙型肝炎合并感染影响的结果。然而,据报道伦敦男男性行为者中丙型肝炎合并感染患者数量有所增加[1],且意大利的传播途径正转向男男性行为者[2],因此了解全球范围内艾滋病的发展和管理情况对于规划未来服务很重要。英国队列显示需要入院治疗的疾病范围更广,且随着艾滋病患者群体老龄化,预计未来这一情况会增加,这需要普通和专科艾滋病医生密切合作。根据英国艾滋病协会(BHIVA)2012年指南[3],艾滋病病毒RNA阈值为400拷贝/毫升以解释波动情况。