Overend Karen, Lewis Helen, Bailey Della, Bosanquet Kate, Chew-Graham Carolyn, Ekers David, Gascoyne Samantha, Hems Deborah, Holmes John, Keding Ada, McMillan Dean, Meer Shaista, Meredith Jodi, Mitchell Natasha, Nutbrown Sarah, Parrott Steve, Richards David, Traviss Gemma, Trépel Dominic, Woodhouse Rebecca, Gilbody Simon
Department of Health Sciences, University of York, Seebohm Rowntree, Building, Heslington, York YO10 5DD, UK.
Trials. 2014 Nov 19;15(1):451. doi: 10.1186/1745-6215-15-451.
Depression accounts for the greatest disease burden of all mental health disorders, contributes heavily to healthcare costs, and by 2020 is set to become the second largest cause of global disability. Although 10% to 16% of people aged 65 years and over are likely to experience depressive symptoms, the condition is under-diagnosed and often inadequately treated in primary care. Later-life depression is associated with chronic illness and disability, cognitive impairment and social isolation. With a progressively ageing population it becomes increasingly important to refine strategies to identity and manage depression in older people. Currently, management may be limited to the prescription of antidepressants where there may be poor concordance; older people may lack awareness of psychosocial interventions and general practitioners may neglect to offer this treatment option.
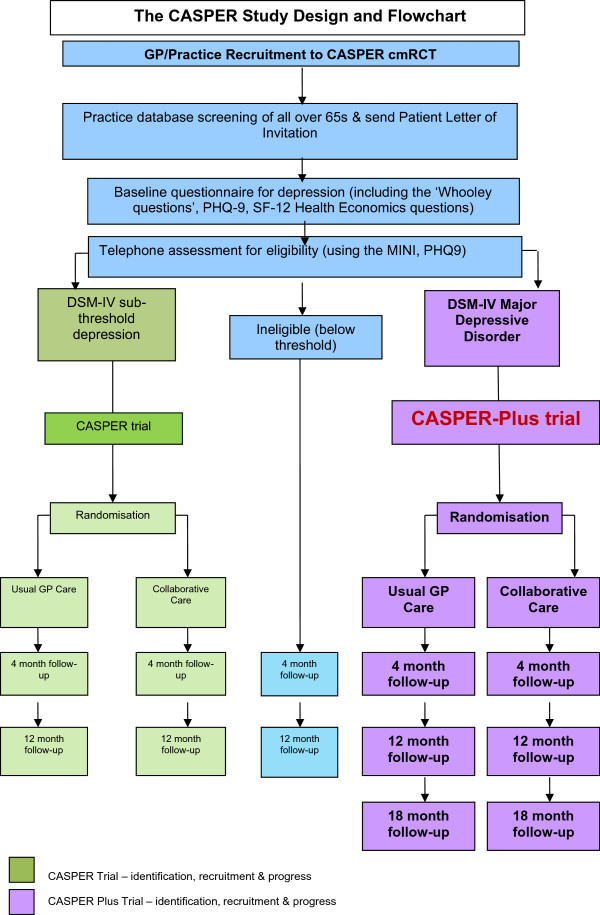
METHODS/DESIGN: CASPER Plus is a multi-centre, randomised controlled trial of a collaborative care intervention for individuals aged 65 years and over experiencing moderate to severe depression. Selected practices in the North of England identify potentially eligible patients and invite them to participate in the study. A diagnostic interview is carried out and participants with major depressive disorder are randomised to either collaborative care or usual care. The recruitment target is 450 participants. The intervention, behavioural activation and medication management in a collaborative care framework, has been adapted to meet the complex needs of older people. It is delivered over eight to 10 weekly sessions by a case manager liaising with general practitioners. The trial aims to evaluate the clinical and cost effectiveness of collaborative care in addition to usual GP care versus usual GP care alone. The primary clinical outcome, depression severity, will be measured with the Patient Health Questionnaire-9 (PHQ-9) at baseline, 4, 12 and 18 months. Cost effectiveness analysis will assess health-related quality of life using the SF-12 and EQ-5D and will examine cost-consequences of collaborative care. A qualitative process evaluation will be undertaken to explore acceptability, gauge the extent to which the intervention is implemented and to explore sustainability beyond the clinical trial.
Results will add to existing evidence and a positive outcome may lead to the commissioning of this model of service in primary care.
ISRCTN45842879 (24 July 2012).
抑郁症是所有心理健康障碍中疾病负担最重的,对医疗成本有很大影响,到2020年将成为全球残疾的第二大原因。虽然65岁及以上的人群中有10%至16%可能会出现抑郁症状,但在初级保健中,这种情况诊断不足且治疗往往不充分。晚年抑郁症与慢性病和残疾、认知障碍及社会隔离有关。随着人口老龄化的加剧,完善识别和管理老年人抑郁症的策略变得越来越重要。目前,管理可能仅限于开具抗抑郁药,但患者的依从性可能较差;老年人可能对心理社会干预缺乏认识,而全科医生可能会忽略提供这种治疗选择。
方法/设计:CASPER Plus是一项针对65岁及以上患有中度至重度抑郁症个体的协作式护理干预的多中心随机对照试验。英格兰北部选定的医疗机构识别出可能符合条件的患者,并邀请他们参与研究。进行诊断访谈,患有重度抑郁症的参与者被随机分配到协作式护理组或常规护理组。招募目标是450名参与者。在协作式护理框架下的干预措施,即行为激活和药物管理,已进行调整以满足老年人的复杂需求。由一名与全科医生联络的个案管理员通过每周八至十次的疗程来实施。该试验旨在评估除常规全科医生护理外协作式护理与单纯常规全科医生护理相比的临床效果和成本效益。主要临床结局,即抑郁严重程度,将在基线、4个月、12个月和18个月时使用患者健康问卷-9(PHQ-9)进行测量。成本效益分析将使用SF-12和EQ-5D评估与健康相关的生活质量,并将研究协作式护理的成本后果。将进行定性过程评估,以探讨可接受性、衡量干预措施的实施程度,并探索临床试验之外的可持续性。
结果将补充现有证据,积极的结果可能会促使在初级保健中采用这种服务模式。
ISRCTN45842879(2012年7月24日)。