Ogba Ndiya, Manning Nicole G, Bliesner Brian S, Ambler S Kelly, Haughian James M, Pinto Mauricio P, Jedlicka Paul, Joensuu Kristiina, Heikkilä Päivi, Horwitz Kathryn B
Department of Medicine, University of Colorado Anschutz Medical Campus, 12801 E. 7th Avenue, Aurora, CO, 80045, USA.
Department of Pathology, University of Colorado Anschutz Medical Campus, 12801 E. 7th Avenue, Aurora, CO, 80045, USA.
Breast Cancer Res. 2014 Dec 5;16(6):489. doi: 10.1186/s13058-014-0489-4.
Luminal, estrogen receptor-positive (ER(+)) breast cancers can metastasize but lie dormant for years before recurrences prove lethal. Understanding the roles of estrogen (E) or progestin (P) in development of luminal metastases or in arousal from dormancy is hindered by few preclinical models. We have developed such models.
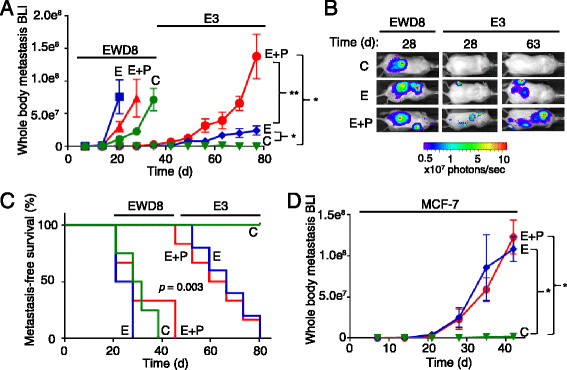
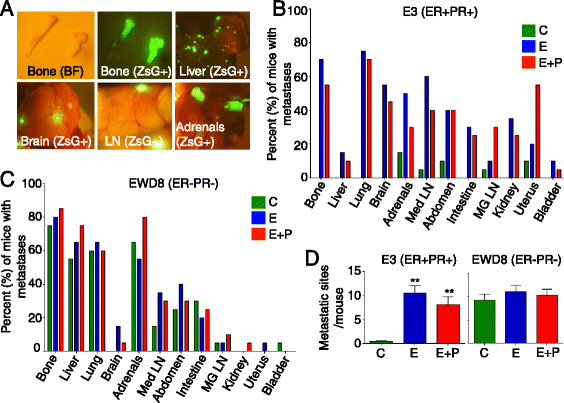
Immunocompromised, ovariectomized (ovx'd) mice were intracardiac-injected with luminal or basal human breast cancer cells. Four lines were tested: luminal ER(+)PR(+) cytokeratin 5-negative (CK5(-)) E3 and MCF-7 cells, basal ER(-)PR(-)CK5(+) estrogen withdrawn-line 8 (EWD8) cells, and basal ER(-)PR(-)CK5(-) MDA-MB-231 cells. Development of micrometastases or macrometastases was quantified in ovx'd mice and in mice supplemented with E or P or both. Metastatic deposits were analyzed by immunohistochemistry for luminal, basal, and proliferation markers.
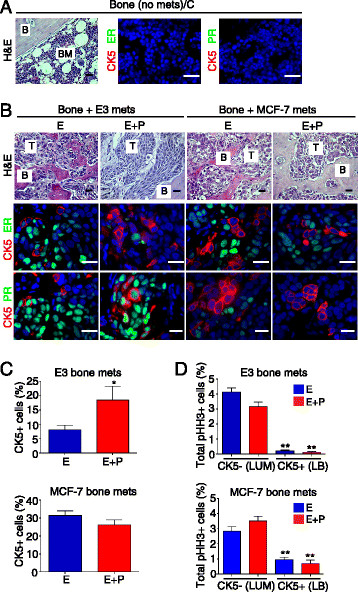
ER(-)PR(-) cells generated macrometastases in multiple organs in the absence or presence of hormones. By contrast, ovx'd mice injected with ER(+)PR(+) cells appeared to be metastases-free until they were supplemented with E or E+P. Furthermore, unlike parental ER(+)PR(+)CK5(-) cells, luminal metastases were heterogeneous, containing a significant (6% to 30%) proportion of non-proliferative ER(-)PR(-)CK5(+) cells that would be chemotherapy-resistant. Additionally, because these cells lack receptors, they would also be endocrine therapy-resistant. With regard to ovx'd control mice injected with ER(+)PR(+) cells that appeared to be metastases-free, systematic pathologic analysis of organs showed that some harbor a reservoir of dormant micrometastases that are ER(+) but PR(-). Such cells may also be endocrine therapy- and chemotherapy-resistant. Their emergence as macrometastases can be triggered by E or E+P restoration.
We conclude that hormones promote development of multi-organ macrometastases in luminal disease. The metastases display a disturbing heterogeneity, containing newly emergent ER(-)PR(-) subpopulations that would be resistant to endocrine therapy and chemotherapy. Similar cells are found in luminal metastases of patients. Furthermore, lack of hormones is not protective. While no overt metastases form in ovx'd mice, luminal tumor cells can seed distant organs, where they remain dormant as micrometastases and sheltered from therapies but arousable by hormone repletion. This has implications for breast cancer survivors or women with occult disease who are prescribed hormones for contraception or replacement purposes.
管腔型雌激素受体阳性(ER(+))乳腺癌可发生转移,但在复发证明致命之前会潜伏数年。由于临床前模型较少,雌激素(E)或孕激素(P)在管腔型转移瘤发生或从休眠状态激活过程中的作用尚不清楚。我们已建立了此类模型。
对免疫缺陷、卵巢切除(ovx'd)的小鼠进行心内注射管腔型或基底型人乳腺癌细胞。测试了四条细胞系:管腔型ER(+)PR(+)细胞角蛋白5阴性(CK5(-))的E3和MCF-7细胞、基底型ER(-)PR(-)CK5(+)雌激素撤除8号线(EWD8)细胞,以及基底型ER(-)PR(-)CK5(-)的MDA-MB-231细胞。在ovx'd小鼠以及补充E或P或两者的小鼠中对微转移瘤或大转移瘤的发生情况进行定量分析。通过免疫组织化学分析转移灶中的管腔型、基底型和增殖标志物。
ER(-)PR(-)细胞在有无激素的情况下均可在多个器官中形成大转移瘤。相比之下,注射了ER(+)PR(+)细胞的ovx'd小鼠在补充E或E+P之前似乎没有转移瘤。此外,与亲代ER(+)PR(+)CK5(-)细胞不同,管腔型转移瘤具有异质性,含有相当比例(6%至30%)的非增殖性ER(-)PR(-)CK5(+)细胞,这些细胞对化疗具有抗性。此外,由于这些细胞缺乏受体,它们也对内分泌治疗具有抗性。对于注射了ER(+)PR(+)细胞且似乎没有转移瘤的ovx'd对照小鼠,对器官进行的系统病理分析表明,一些器官中存在休眠微转移瘤库,这些微转移瘤为ER(+)但PR(-)。此类细胞也可能对内分泌治疗和化疗具有抗性。E或E+P恢复可触发它们发展为大转移瘤。
我们得出结论,激素促进管腔型疾病中多器官大转移瘤的形成。转移瘤表现出令人不安的异质性,包含新出现的ER(-)PR(-)亚群,这些亚群对内分泌治疗和化疗具有抗性。在患者的管腔型转移瘤中也发现了类似的细胞。此外,缺乏激素并无保护作用。虽然ovx'd小鼠中未形成明显的转移瘤,但管腔型肿瘤细胞可在远处器官着床,在那里它们作为微转移瘤保持休眠状态,免受治疗影响,但可因激素补充而激活。这对乳腺癌幸存者或患有隐匿性疾病且因避孕或替代目的而服用激素的女性具有重要意义。