Paediatric Endocrinology Department , John Hunter Children's Hospital , Newcastle, New South Wales , Australia ; Faculty of Health and Medicine , The University of Newcastle , Newcastle, New South Wales , Australia ; Hunter Medical Research Institute , Newcastle, New South Wales , Australia.
AIM Diabetes Centre , Newcastle, New South Wales , Australia.
BMJ Open Diabetes Res Care. 2014 Dec 4;2(1):e000050. doi: 10.1136/bmjdrc-2014-000050. eCollection 2014.
Insulin pumps are able to deliver bolus insulin as a standard, extended or combination bolus. There is minimal research to determine which bolus is preferable in different settings. Anecdotally, many patients utilizes only the standard bolus (SB) due to uncertainty regarding when and how to program the different bolus types. We compared postprandial glycemia when five different extended boluses (EBs) and an SB were used following a test meal. We sought to determine the impact of varying rates of insulin delivery from an EB on early postprandial glycemia.
We conducted a randomized, repeated measures trial of 20 children and adults comparing postprandial glycemic excursions following EBs given at five different rates with SB as a control. All EBs were delivered over 2 h. Rates of EBs were chosen to reflect EBs used in clinical practice: EB1HR=100% of insulin:carbohydrate ratio (ICR) per hour (200% ICR total dose); EB2HR=50% of ICR per hour; EB3HR=33% of ICR per hour; EB4HR=25% of ICR per hour; EB6HR=16% ICR per hour. A standardized breakfast was given and activity was standardized. Continuous glucose monitoring was used to assess glycemia for 2 h after the meal.
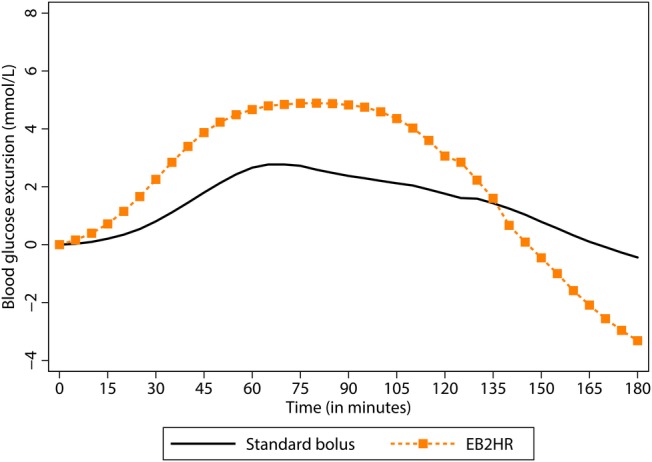
The mean postprandial glycemic excursions were lower at 30, 60, and 90 min (p<0.05) for SB compared with all EBs. The mean peak postprandial glycemic excursion and the area under the curve was lower for SB compared with all EBs (p<0.05).
EBs resulted in higher postprandial glycemic excursions than SB for 2 h after the meal. For a moderate glycemic index meal EBs are unable to control glycemia for 2 h after a meal as well as SB. Further studies with different meal types are required to determine the impact of differential delivery of the EB on postprandial glycemia.
ACTRN12612000609853.
胰岛素泵能够提供标准、延长或组合的推注胰岛素。在不同的情况下,哪种推注更优,研究甚少。据推测,由于不确定何时以及如何编程不同类型的推注,许多患者仅使用标准推注 (SB)。我们比较了不同的延长推注 (EB) 和 SB 在餐后 2 小时的血糖控制效果。我们试图确定不同的 EB 胰岛素输送率对餐后早期血糖的影响。
我们进行了一项随机、重复测量的试验,比较了 20 名儿童和成人在接受不同速率的 EB 推注和 SB 控制后的餐后血糖波动。所有的 EB 都是在 2 小时内输注的。选择 EB 的速率以反映临床实践中使用的 EB:EB1HR=每小时胰岛素:碳水化合物比例 (ICR) 的 100%(总剂量为 200% ICR);EB2HR=每小时 ICR 的 50%;EB3HR=每小时 ICR 的 33%;EB4HR=每小时 ICR 的 25%;EB6HR=每小时 ICR 的 16%。给予标准化早餐,标准化活动。连续血糖监测用于评估餐后 2 小时内的血糖。
与所有 EB 相比,SB 在 30、60 和 90 分钟时餐后血糖波动较低(p<0.05)。与所有 EB 相比,SB 的餐后血糖峰值和曲线下面积较低(p<0.05)。
与 SB 相比,EB 在餐后 2 小时内导致更高的餐后血糖波动。对于中血糖指数的餐食,EB 在餐后 2 小时内无法像 SB 那样控制血糖。需要进一步研究不同类型的餐食,以确定 EB 的不同输送对餐后血糖的影响。
ACTRN12612000609853。