Okoli Ugo, Morris Laura, Oshin Adetokunbo, Pate Muhammad A, Aigbe Chidimma, Muhammad Ado
SURE-P MCH Project Implementation Unit, National Primary Health Care Development Agency, Abuja, Nigeria.
Duke Global Health Institute, Duke University, Durham, USA.
BMC Pregnancy Childbirth. 2014 Dec 12;14:408. doi: 10.1186/s12884-014-0408-9.
This paper describes use of a Conditional Cash Transfer (CCT) programme to encourage use of critical MNCH services among rural women in Nigeria.
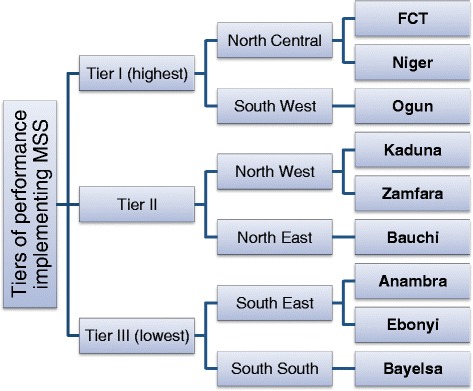
The CCT programme was first implemented as a pilot in 37 primary health care facilities (PHCs), in nine Nigerian states. The programme entitles women using these facilities up to N5,000 (approximately US$30) if they attend antenatal care (ANC), skilled delivery, and postnatal care. There are 88 other PHCs from these nine states included in this study, which implemented a standard package of supply upgrades without the CCT. Data on monthly service uptake throughout the continuum of care was collected at 124 facilities during quarterly monitoring visits. An interrupted time series using segmented linear regression was applied to estimate separately the effects of the CCT programme and supply package on service uptake.
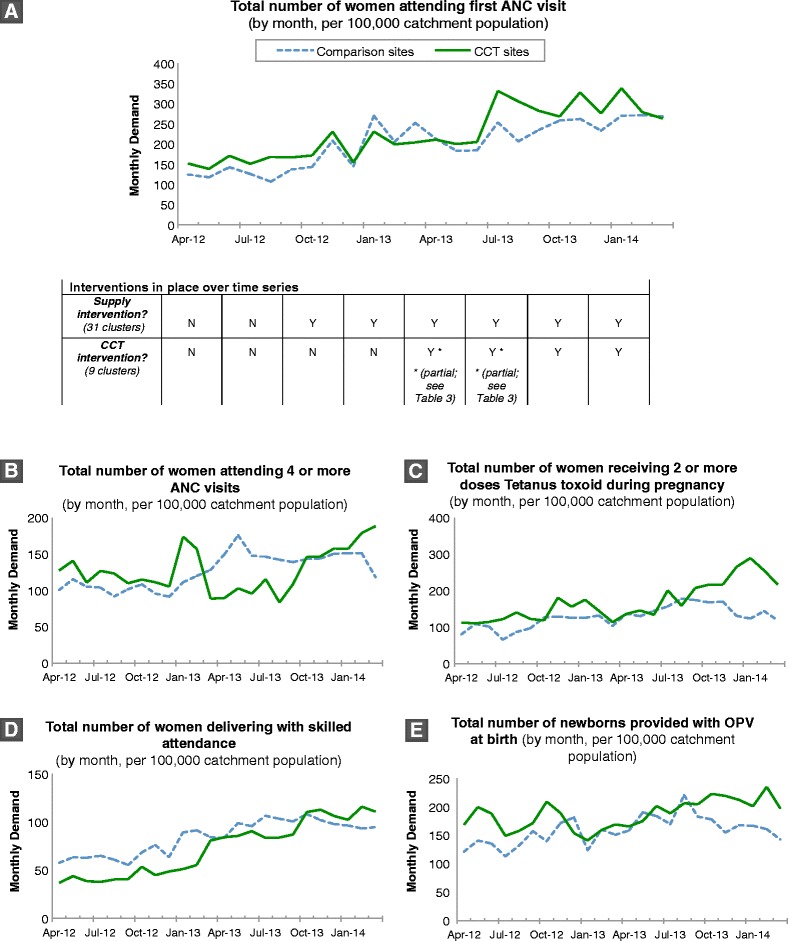
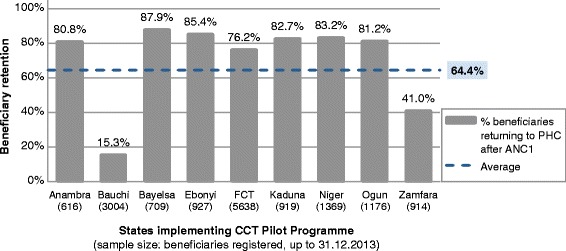
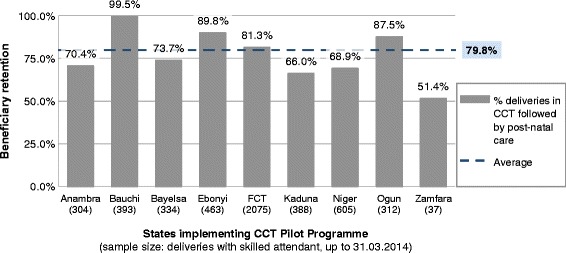
From April 2013-March 2014, 20,133 women enrolled in the CCT. Sixty-four percent of beneficiaries returned at least once after registration, and 80% of women delivering with skilled attendance returned after delivery. The CCT intervention is associated with a statistically significant increase in the monthly number of women attending four or more ANC visits (increase of 15.12 visits per 100,000 catchment population, p < 0.01; 95% confidence interval 7.38 to 22.85), despite a negative level effect immediately after the intervention began (-45.53/100,000 catchment population; p < 0.05; 95% CI -82.71 to -8.36). A statistically significant increase was also observed in the monthly number of women receiving two or more Tetanus toxoid doses during pregnancy (21.65/100,000 catchment population; p < 0.01; 95% CI 9.23 to 34.08). Changes for other outcomes with the CCT intervention (number of women attending first ANC visit; number of deliveries with skilled attendance; number of neonates receiving OPV at birth) were not found to be statistically significant.
The results show that the CCT intervention is capable of significant effects on service uptake, although results for several outcomes of interest were inconclusive. Key lessons learnt from the pilot phase of implementation include a need to track beneficiary retention throughout the continuum of care as closely as possible, and avert loss to follow-up.
本文描述了使用有条件现金转移支付(CCT)计划来鼓励尼日利亚农村妇女使用关键的妇幼保健服务。
CCT计划于2013年4月至2014年3月在尼日利亚九个州的37个初级卫生保健机构(PHC)作为试点首次实施。该计划规定,如果妇女接受产前护理(ANC)、熟练接生和产后护理,使用这些机构的妇女可获得高达5000奈拉(约合30美元)。本研究纳入了这九个州的另外88个PHC,它们实施了一套标准的供应升级方案,但没有CCT。在季度监测访问期间,在124个机构收集了整个连续护理过程中每月服务利用情况的数据。使用分段线性回归的中断时间序列分别用于估计CCT计划和供应包对服务利用的影响。
2013年4月至2014年3月,有20133名妇女参加了CCT。64%的受益人在登记后至少回访过一次,80%有熟练接生服务的产妇在分娩后回访。CCT干预与每月参加四次或更多次ANC访视的妇女人数在统计学上显著增加相关(每10万服务人口增加15.12次访视,p<0.01;95%置信区间7.38至22.85),尽管在干预开始后立即出现了负的水平效应(-45.53/10万服务人口;p<0.05;95%CI -82.71至-8.36)。在孕期接受两剂或更多剂破伤风类毒素的妇女人数每月也有统计学上的显著增加(21.65/10万服务人口;p<0.01;95%CI 9.23至34.08)。未发现CCT干预对其他结果(首次参加ANC访视的妇女人数;有熟练接生服务的分娩次数;出生时接受口服脊髓灰质炎疫苗的新生儿人数)的变化具有统计学意义。
结果表明,CCT干预能够对服务利用产生显著影响,尽管几个感兴趣的结果的结果尚无定论。从试点实施阶段吸取的主要经验教训包括需要尽可能密切地跟踪整个连续护理过程中的受益人留存情况,并避免失访。