Gabbe Belinda J, Simpson Pam M, Lyons Ronan A, Ameratunga Shanthi, Harrison James E, Derrett Sarah, Polinder Suzanne, Davie Gabrielle, Rivara Frederick P
Department of Epidemiology and Preventive Medicine, Monash University, Melbourne, Australia; Centre for Improvement of Population Health through E-records Research, Swansea University, Swansea, United Kingdom.
Department of Epidemiology and Preventive Medicine, Monash University, Melbourne, Australia.
PLoS One. 2014 Dec 11;9(12):e113467. doi: 10.1371/journal.pone.0113467. eCollection 2014.
To determine associations between the number of injuries sustained and three measures of disability 12-months post-injury for hospitalised patients.
Data from 27,840 adult (18+ years) participants, hospitalised for injury, were extracted for analysis from the Validating and Improving injury Burden Estimates (Injury-VIBES) Study. Modified Poisson and linear regression analyses were used to estimate relative risks and mean differences, respectively, for a range of outcomes (Glasgow Outcome Scale-Extended, GOS-E; EQ-5D and 12-item Short Form health survey physical and mental component summary scores, PCS-12 and MCS-12) according to the number of injuries sustained, adjusted for age, sex and contributing study.
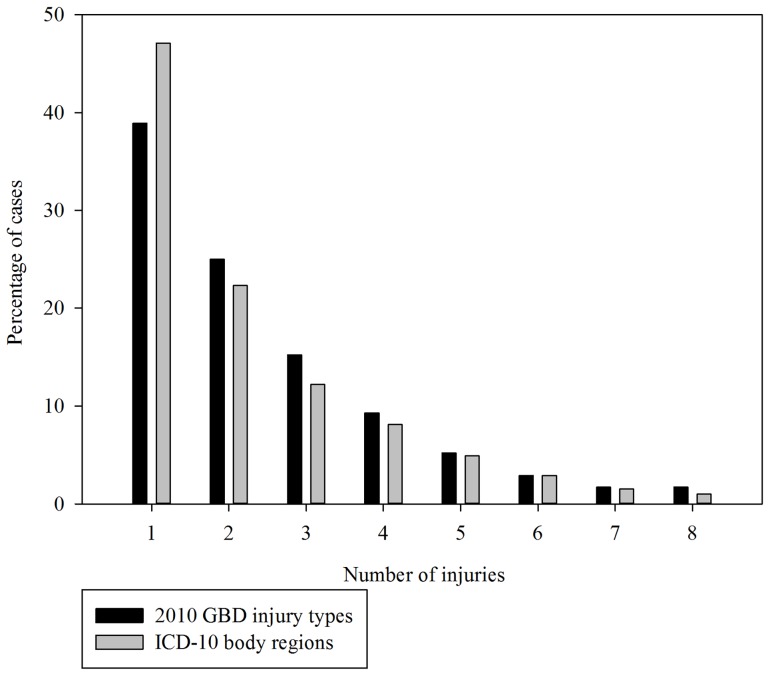
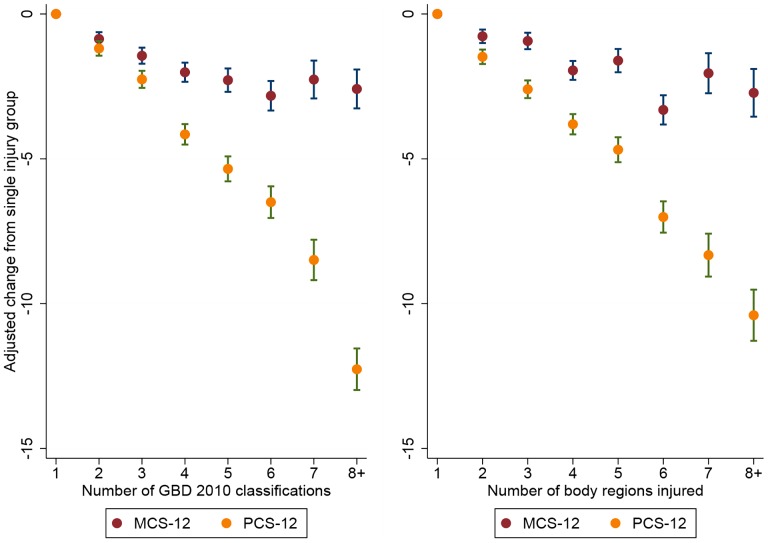
More than half (54%) of patients had an injury to more than one ICD-10 body region and 62% had sustained more than one Global Burden of Disease injury type. The adjusted relative risk of a poor functional recovery (GOS-E<7) and of reporting problems on each of the items of the EQ-5D increased by 5-10% for each additional injury type, or body region, injured. Adjusted mean PCS-12 and MCS-12 scores worsened with each additional injury type, or body region, injured by 1.3-1.5 points and 0.5 points, respectively.
Consistent and strong relationships exist between the number of injury types and body regions injured and 12-month functional and health status outcomes. Existing composite measures of anatomical injury severity such as the NISS or ISS, which use up to three diagnoses only, may be insufficient for characterising or accounting for multiple injuries in disability studies. Future studies should consider the impact of multiple injuries to avoid under-estimation of injury burden.
确定住院患者受伤数量与受伤后12个月三种残疾衡量指标之间的关联。
从“验证和改进伤害负担估计(Injury-VIBES)研究”中提取了27840名因伤住院的成年(18岁及以上)参与者的数据进行分析。采用修正泊松回归和线性回归分析,分别根据受伤数量估计一系列结局(扩展格拉斯哥结局量表,GOS-E;EQ-5D以及12项简短健康调查问卷身体和心理成分汇总得分,PCS-12和MCS-12)的相对风险和平均差异,并对年龄、性别和参与研究进行了调整。
超过一半(54%)的患者有超过一个国际疾病分类第十版(ICD-10)身体部位受伤,62%的患者遭受了不止一种全球疾病负担伤害类型。每增加一种受伤类型或身体部位,功能恢复不佳(GOS-E<7)以及在EQ-5D各项目上报告问题的调整后相对风险增加5%-10%。随着每增加一种受伤类型或身体部位,调整后的平均PCS-12和MCS-12得分分别恶化1.3-1.5分和0.5分。
受伤类型和身体部位数量与12个月功能和健康状况结局之间存在一致且强烈的关系。现有的解剖学损伤严重程度综合衡量指标,如仅使用多达三个诊断的简明损伤定级标准(AIS)或损伤严重程度评分(ISS),在残疾研究中可能不足以描述或解释多处损伤。未来的研究应考虑多处损伤的影响,以避免低估伤害负担。