Singh Abha G, Kermani Tanaz A, Crowson Cynthia S, Weyand Cornelia M, Matteson Eric L, Warrington Kenneth J
From the Division of Rheumatology, Mayo Clinic, Rochester, Minnesota; Division of Rheumatology, University of California, Los Angeles; Division of Immunology and Rheumatology, Stanford University School of Medicine, Stanford, California, USA.A.G. Singh, MBBS, Division of Rheumatology, Mayo Clinic; T.A. Kermani, MD, MS, Division of Rheumatology, University of California, Los Angeles; C.S. Crowson, MS, Division of Rheumatology, Mayo Clinic; C.M. Weyand, MD, PhD, Division of Immunology and Rheumatology, Stanford University School of Medicine; E.L. Matteson, MD, MPH; K.J. Warrington, MD, Division of Rheumatology, Mayo Clinic.
J Rheumatol. 2015 Feb;42(2):309-15. doi: 10.3899/jrheum.140188. Epub 2014 Dec 15.
To evaluate clinical characteristics, treatment, and outcomes of patients with visual changes from giant cell arteritis (GCA) and to examine trends over the last 5 decades.
We reviewed the medical records of a population-based cohort of patients with GCA diagnosed between 1950 and 2004. The clinical, ophthalmological, and laboratory features of patients with visual manifestations attributable to GCA were compared to patients without visual complications. Trends over time were examined using logistic regression modeling adjusted for age and sex.
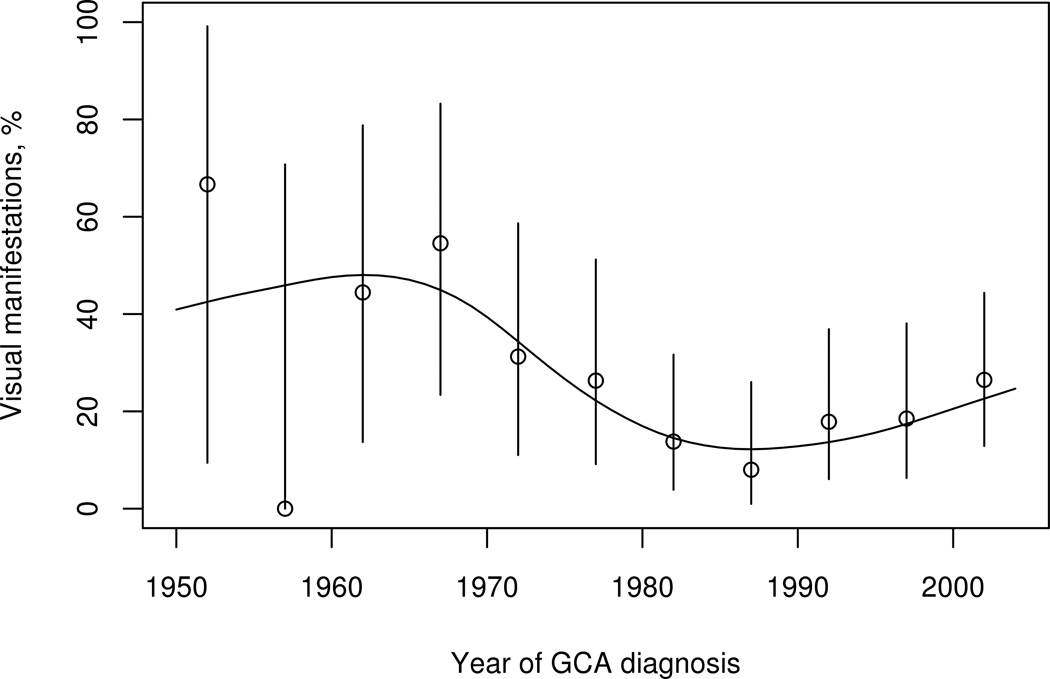
In a cohort of 204 cases of GCA (mean age 76.0 ± 8.2 yrs, 80% female), visual changes from GCA were observed in 47 patients (23%), and 4.4% suffered complete vision loss. A higher proportion of patients with visual manifestations reported jaw claudication than did patients without visual changes (55% vs 38%, p = 0.04). Over a period of 55 years, we observed a significant decline in the incidence of visual symptoms due to GCA. There was a lower incidence of ischemic optic neuropathy in the 1980-2004 cohort vs 1950-1979 (6% vs 15%, p = 0.03). Patients diagnosed in later decades were more likely to recover from visual symptoms (HR 1.34, 95% CI 1.06-1.71). Chances of recovery were poor in patients with anterior ischemic optic neuropathy or complete vision loss.
Incidence of visual symptoms has declined over the past 5 decades, and chances of recovery from visual symptoms have improved. However, complete loss of vision is essentially irreversible. Jaw claudication is associated with higher likelihood of development of visual symptoms.
评估巨细胞动脉炎(GCA)导致视力改变患者的临床特征、治疗及预后,并研究过去50年的变化趋势。
我们回顾了1950年至2004年间确诊的基于人群队列的GCA患者的病历。将GCA所致视力表现患者的临床、眼科和实验室特征与无视力并发症的患者进行比较。使用经年龄和性别调整的逻辑回归模型研究随时间的变化趋势。
在204例GCA患者队列中(平均年龄76.0±8.2岁,80%为女性),47例(23%)出现GCA所致视力改变,4.4%的患者视力完全丧失。有视力表现的患者出现颌部跛行的比例高于无视力改变的患者(55%对38%,p = 0.04)。在55年期间,我们观察到GCA所致视觉症状的发生率显著下降。1980 - 2004年队列中缺血性视神经病变发生率低于1950 - 1979年队列(6%对15%,p = 0.03)。在较后几十年确诊的患者更有可能从视觉症状中恢复(风险比1.34,95%置信区间1.06 - 1.71)。前部缺血性视神经病变或视力完全丧失的患者恢复机会较差。
在过去50年中,视觉症状的发生率有所下降,从视觉症状中恢复的机会有所改善。然而,视力完全丧失基本上是不可逆的。颌部跛行与发生视觉症状的可能性较高相关。