Cassim Naseem, Coetzee Lindi M, Schnippel Kathryn, Glencross Deborah K
National Health Laboratory Service (NHLS), National Priority Programmes, Johannesburg, South Africa.
Health Economics and Epidemiology Research Office, Department of Clinical Medicine, Faculty of Health Sciences, University of Witwatersrand, Johannesburg, South Africa.
PLoS One. 2014 Dec 17;9(12):e115420. doi: 10.1371/journal.pone.0115420. eCollection 2014.
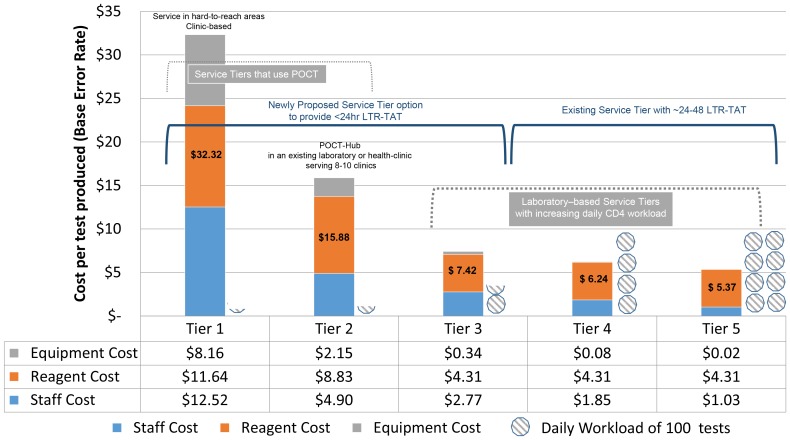
An integrated tiered service delivery model (ITSDM) has been proposed to provide 'full-coverage' of CD4 services throughout South Africa. Five tiers are described, defined by testing volumes and number of referring health-facilities. These include: (1) Tier-1/decentralized point-of-care service (POC) in a single site; Tier-2/POC-hub servicing processing < 30-40 samples from 8-10 health-clinics; Tier-3/Community laboratories servicing ∼ 50 health-clinics, processing < 150 samples/day; high-volume centralized laboratories (Tier-4 and Tier-5) processing < 300 or > 600 samples/day and serving > 100 or > 200 health-clinics, respectively. The objective of this study was to establish costs of existing and ITSDM-tiers 1, 2 and 3 in a remote, under-serviced district in South Africa.
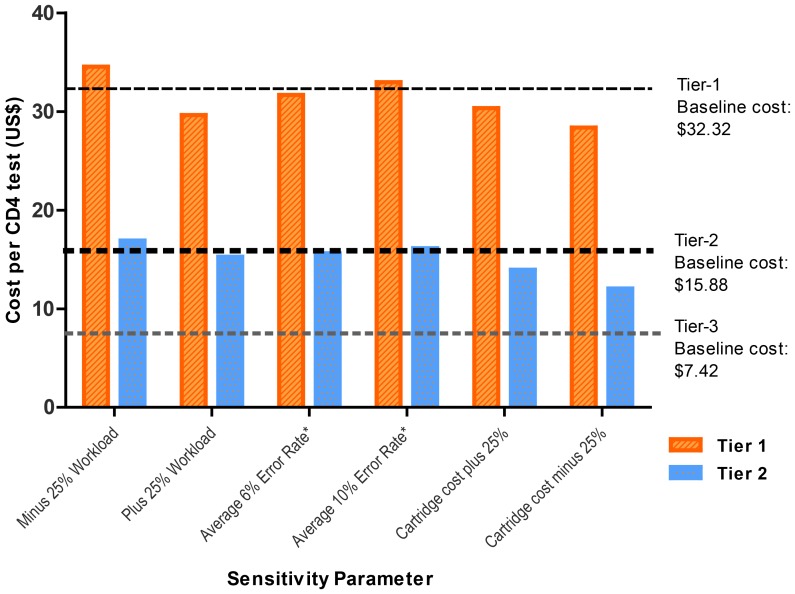
Historical health-facility workload volumes from the Pixley-ka-Seme district, and the total volumes of CD4 tests performed by the adjacent district referral CD4 laboratories, linked to locations of all referring clinics and related laboratory-to-result turn-around time (LTR-TAT) data, were extracted from the NHLS Corporate-Data-Warehouse for the period April-2012 to March-2013. Tiers were costed separately (as a cost-per-result) including equipment, staffing, reagents and test consumable costs. A one-way sensitivity analyses provided for changes in reagent price, test volumes and personnel time.
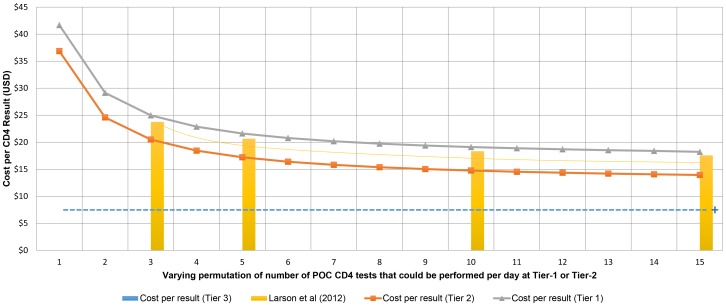
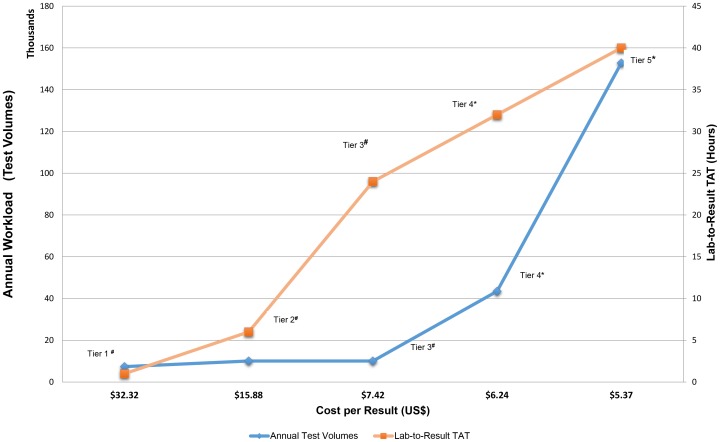
The lowest cost-per-result was noted for the existing laboratory-based Tiers- 4 and 5 ($6.24 and $5.37 respectively), but with related increased LTR-TAT of > 24-48 hours. Full service coverage with TAT < 6-hours could be achieved with placement of twenty-seven Tier-1/POC or eight Tier-2/POC-hubs, at a cost-per-result of $32.32 and $15.88 respectively. A single district Tier-3 laboratory also ensured 'full service coverage' and < 24 hour LTR-TAT for the district at $7.42 per-test.
Implementing a single Tier-3/community laboratory to extend and improve delivery of services in Pixley-ka-Seme, with an estimated local ∼ 12-24-hour LTR-TAT, is ∼ $2 more than existing referred services per-test, but 2-4 fold cheaper than implementing eight Tier-2/POC-hubs or providing twenty-seven Tier-1/POCT CD4 services.
已提出一种综合分层服务提供模式(ITSDM),以在南非全境提供“全面覆盖”的CD4检测服务。该模式描述了五个层级,根据检测量和转诊医疗机构数量来定义。这些层级包括:(1)一级/单站点分散式即时护理服务(POC);二级/POC中心,为8 - 10家健康诊所处理少于30 - 40份样本;三级/社区实验室,为约50家健康诊所服务,每天处理少于150份样本;高容量集中实验室(四级和五级),分别每天处理少于300份或多于600份样本,并为多于100家或多于200家健康诊所服务。本研究的目的是确定南非一个偏远、服务不足地区现有模式以及ITSDM的一级、二级和三级模式的成本。
从国家卫生实验室服务局企业数据仓库中提取了皮克斯利 - 卡 - 塞梅区医疗机构的历史工作量数据,以及相邻地区转诊CD4实验室进行的CD4检测总量,这些数据与所有转诊诊所的位置以及相关的实验室到结果周转时间(LTR - TAT)数据相关,时间段为2012年4月至2013年3月。对各层级分别进行成本核算(以每个结果的成本计算),包括设备、人员、试剂和检测耗材成本。进行了单向敏感性分析,以分析试剂价格、检测量和人员时间的变化。
现有基于实验室的四级和五级模式每个结果的成本最低(分别为6.24美元和5.37美元),但相关的LTR - TAT增加到超过24 - 48小时。通过设置27个一级/POC或8个二级/POC中心可实现TAT < 6小时的全面服务覆盖,每个结果的成本分别为32.32美元和15.88美元。一个区级三级实验室也能确保为该地区提供“全面服务覆盖”且LTR - TAT < 24小时,每次检测成本为7.42美元。
在皮克斯利 - 卡 - 塞梅区设立一个三级/社区实验室以扩展和改善服务提供,预计当地LTR - TAT约为12 - 24小时,每次检测成本比现有转诊服务高出约2美元,但比设立8个二级/POC中心或提供27个一级/POC CD4服务便宜2 - 4倍。