Division of Population Sciences, Dana-Farber Cancer Institute, Boston, Massachusetts, USA
Department of Epidemiology, Harvard T. H. Chan School of Public Health, Boston, MA, United States.
BMJ Glob Health. 2020 Oct;5(10). doi: 10.1136/bmjgh-2020-003493.
Decisions regarding the geographical placement of healthcare services require consideration of trade-offs between equity and efficiency, but few empirical assessments are available. We applied a novel geospatial framework to study these trade-offs in four African countries.
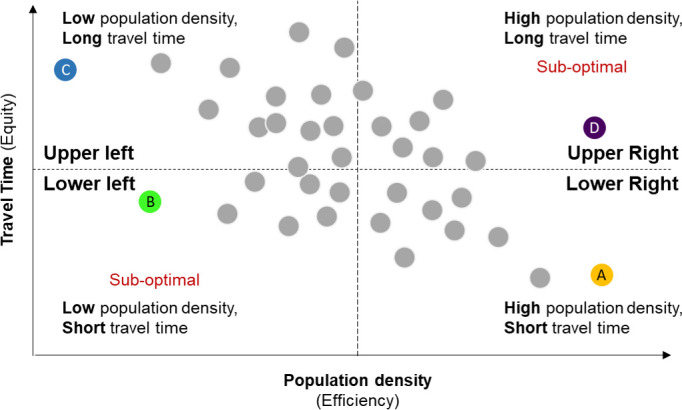
Geolocation data on population density (a surrogate for efficiency), health centres and cancer referral centres in Kenya, Malawi, Tanzania and Rwanda were obtained from online databases. Travel time to the closest facility (a surrogate for equity) was estimated with 1 km resolution using the Access Mod 5 least cost distance algorithm. We studied associations between district-level average population density and travel time to closest facility for each country using Pearson's correlation, and spatial autocorrelation using the Global Moran's I statistic. Geographical clusters of districts with inefficient resource allocation were identified using the bivariate local indicator of spatial autocorrelation.
Population density was inversely associated with travel time for all countries and levels of the health system (Pearson's correlation range, health centres: -0.89 to -0.71; cancer referral centres: -0.92 to -0.43), favouring efficiency. For health centres, negative spatial autocorrelation (geographical clustering of dissimilar values of population density and travel time) was weaker in Rwanda (-0.310) and Tanzania (-0.292), countries with explicit policies supporting equitable access to rural healthcare, relative to Kenya (-0.579) and Malawi (-0.543). Stronger spatial autocorrelation was observed for cancer referral centres (Rwanda: -0.341; Tanzania: -0.259; Kenya: -0.595; Malawi: -0.666). Significant geographical clusters of sparsely populated districts with long travel times to care were identified across countries.
Negative spatial correlations suggested that the geographical distribution of health services favoured efficiency over equity, but spatial autocorrelation measures revealed more equitable geographical distribution of facilities in certain countries. These findings suggest that even when prioritising efficiency, thoughtful decisions regarding geographical allocation could increase equitable physical access to services.
医疗服务的地理位置决策需要考虑公平性和效率之间的权衡,但可供参考的实证评估很少。我们应用了一种新的地理空间框架来研究这四个非洲国家的这些权衡。
从在线数据库中获取肯尼亚、马拉维、坦桑尼亚和卢旺达的人口密度(效率的替代指标)、卫生中心和癌症转诊中心的地理位置数据。使用 Access Mod 5 最小成本距离算法,以 1km 分辨率估算到最近设施的出行时间(公平的替代指标)。我们使用 Pearson 相关系数研究了每个国家的地区平均人口密度与到最近设施的出行时间之间的关联,并用全局 Moran's I 统计量研究了空间自相关。使用二元局部空间自相关指标识别资源分配效率低下的地区的地理聚类。
人口密度与所有国家和卫生系统各级的出行时间呈负相关(Pearson 相关系数范围:卫生中心为-0.89 至-0.71;癌症转诊中心为-0.92 至-0.43),有利于效率。对于卫生中心,卢旺达(-0.310)和坦桑尼亚(-0.292)的负空间自相关(人口密度和出行时间的相似值的地理聚类)较弱,这两个国家都有明确的政策支持农村医疗保健的公平获取,与肯尼亚(-0.579)和马拉维(-0.543)相比。癌症转诊中心的空间自相关更强(卢旺达:-0.341;坦桑尼亚:-0.259;肯尼亚:-0.595;马拉维:-0.666)。在各国之间都发现了存在大量人口稀少且出行时间长的地区的显著地理聚类。
负空间相关性表明,卫生服务的地理分布偏向于效率而不是公平,但空间自相关度量揭示了某些国家设施的地理分布更加公平。这些发现表明,即使在优先考虑效率的情况下,关于地理位置分配的深思熟虑的决策也可以增加公平的服务物理可及性。