Song Seung-Hoon, Roh Hong Gee, Kim Hahn Young, Choi Jin Woo, Moon Won-Jin, Choe Woo Jin, Jung Ileok
Department of Neurology, Konkuk University School of Medicine, Neungdong-ro 120-1, Gwangjin-gu, Seoul, Republic of Korea.
Department of Radiology, Konkuk University School of Medicine, Neungdong-ro 120-1, Gwangjin-gu, Seoul, Republic of Korea.
BMC Neurol. 2014 Dec 18;14:252. doi: 10.1186/s12883-014-0252-6.
Structural anomaly of the cervical spine or craniocervical junction has been reported as one of the rare causes of ischemic stroke. We report a case of a young patient with recurrent posterior circulation infarction that may have been associated with an anomalous occipital bony process compressing the vertebral artery.
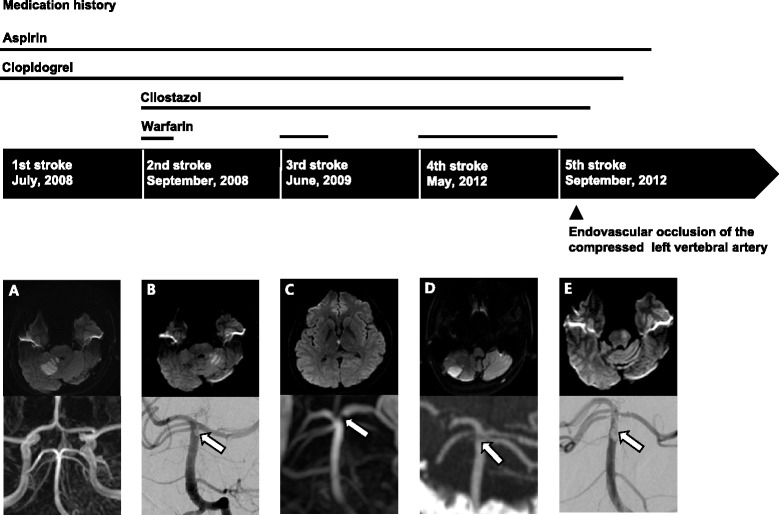
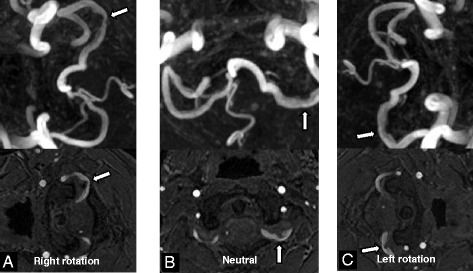
A 23-year-old man experienced recurrent posterior circulation infarction 5 times over a period of 5 years. He had no conventional vascular risk factors. Young age stroke work-up including thorough cardiac, intra- and extracranial vascular evaluation and laboratory tests for the hypercoagulable state or connective tissue disease yielded unremarkable results. An anomalous bony process from the occipital base compressing the left vertebral artery was observed on brain CT. All the recurrent strokes were explainable by the arterial thromboembolism originating from the compressed left vertebral artery. Therefore, the left vertebral artery compressed by the anomalous occipital bony process may have been the culprit behind the recurrent thromboembolic strokes in our patient. Intractable recurrent strokes even under optimal medical treatment led us to make a decision for the intervention. Instead of surgical removal of the anomalous occipital bony process, the left vertebral artery was occluded permanently by endovascular coiling after confirming that this would cause no neurological deficits or flow disturbance in the posterior circulation. There was no recurrence of stroke for 2 years after permanent occlusion of the left vertebral artery.
Arterial thromboembolism originating from the left vertebral artery compressed by the anomalous occipital bony process is a rare but not to be overlooked cause of posterior circulation infarction. When intractable to medical treatment, endovascular occlusion of the vertebral artery without flow disturbance to the posterior circulation may be a useful treatment option when surgical removal is not feasible.
颈椎或颅颈交界处的结构异常已被报道为缺血性中风的罕见原因之一。我们报告一例年轻患者,其反复发生后循环梗死,可能与异常的枕骨骨质压迫椎动脉有关。
一名23岁男性在5年期间反复发生5次后循环梗死。他没有传统的血管危险因素。对年轻患者进行的中风检查,包括全面的心脏、颅内和颅外血管评估以及针对高凝状态或结缔组织疾病的实验室检查,结果均无异常。脑部CT显示枕骨基部有一个异常的骨质压迫左椎动脉。所有反复发生的中风都可以用源自受压左椎动脉的动脉血栓栓塞来解释。因此,被异常枕骨骨质压迫的左椎动脉可能是我们患者反复发生血栓栓塞性中风的罪魁祸首。即使在最佳药物治疗下仍顽固复发的中风促使我们决定进行干预。在确认永久性闭塞左椎动脉不会导致后循环神经功能缺损或血流紊乱后,通过血管内栓塞术将其永久闭塞,而不是手术切除异常的枕骨骨质。左椎动脉永久性闭塞后2年未再发生中风。
源自被异常枕骨骨质压迫的左椎动脉的动脉血栓栓塞是后循环梗死的一种罕见但不可忽视的原因。当药物治疗无效时,在手术切除不可行的情况下,对椎动脉进行无后循环血流紊乱的血管内闭塞可能是一种有效的治疗选择。