Saliba Faouzi, Pascher Andreas, Cointault Olivier, Laterre Pierre-François, Cervera Carlos, De Waele Jan J, Cillo Umberto, Langer Róbert M, Lugano Manuela, Göran-Ericzon Bo, Phillips Stephen, Tweddle Lorraine, Karas Andreas, Brown Malcolm, Fischer Lutz
Hôpital Paul Brousse, Villejuif, France.
Charite Universitätsmedizin, Berlin, Germany.
Clin Infect Dis. 2015 Apr 1;60(7):997-1006. doi: 10.1093/cid/ciu1128. Epub 2014 Dec 17.
Invasive fungal infection (IFI) following liver transplant is associated with significant morbidity and mortality. Antifungal prophylaxis is rational for liver transplant patients at high IFI risk.
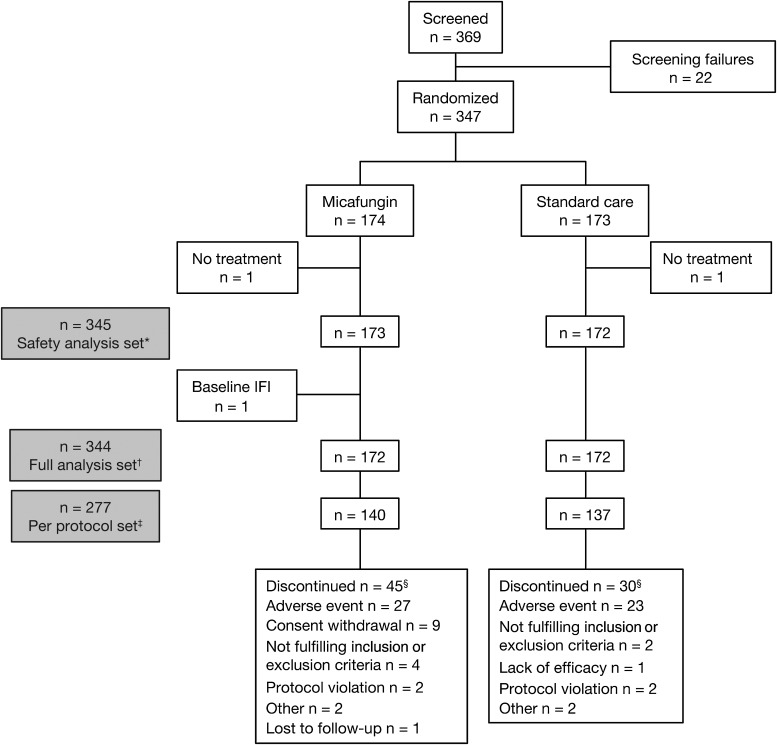
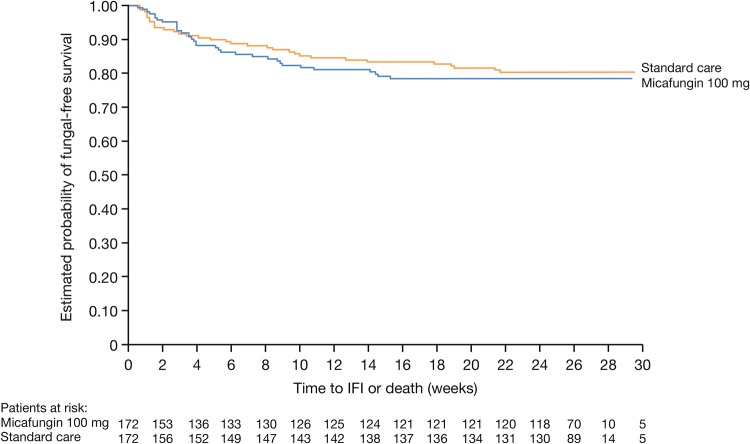
In this open-label, noninferiority study, patients were randomized 1:1 to receive intravenous micafungin 100 mg or center-specific standard care (fluconazole, liposomal amphotericin B, or caspofungin) posttransplant. The primary endpoint was clinical success (absence of a proven/probable IFI and no need for additional antifungals) at end of prophylaxis (EOP). Noninferiority (10% margin) of micafungin vs standard care was assessed in the per protocol and full analysis sets. Safety assessments included adverse events and liver and kidney function tests.
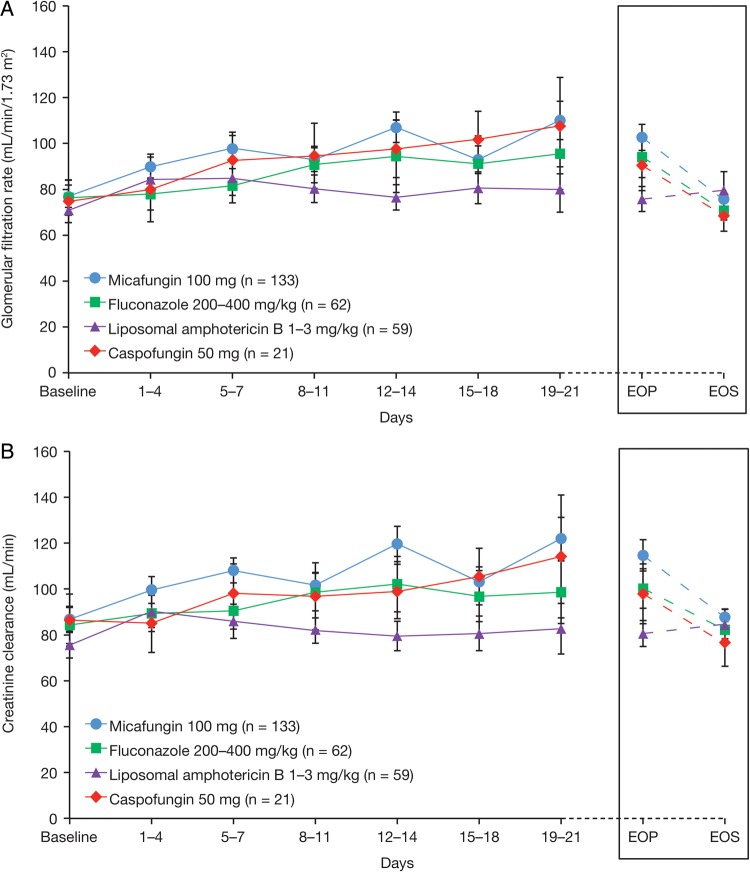
The full analysis set comprised 344 patients (172 micafungin; 172 standard care). Mean age was 51.2 years; 48.0% had a Model for End-Stage Liver Disease score ≥20. At EOP (mean treatment duration, 17 days), clinical success was 98.6% for micafungin and 99.3% for standard care (Δ standard care - micafungin [95% confidence interval], 0.7% [-2.7% to 4.4%]) in the per protocol set and 96.5% and 93.6%, respectively (-2.9% [-8.0% to 1.9%]), in the full analysis set. Incidences of drug-related adverse events for micafungin and standard care were 11.6% and 16.3%, leading to discontinuation in 6.4% and 11.6% of cases, respectively. At EOP, liver function tests were similar but creatinine clearance was higher in micafungin- vs standard care-treated patients.
Micafungin was noninferior to standard care as antifungal prophylaxis in liver transplant patients at high risk for IFI. Adverse event profiles and liver function at EOP were similar, although kidney function was better with micafungin.
NCT01058174.
肝移植后侵袭性真菌感染(IFI)与显著的发病率和死亡率相关。对于IFI高风险的肝移植患者,抗真菌预防是合理的。
在这项开放标签、非劣效性研究中,患者按1:1随机分组,在移植后接受静脉注射米卡芬净100mg或中心特异性标准治疗(氟康唑、脂质体两性霉素B或卡泊芬净)。主要终点是预防结束时(EOP)的临床成功(无确诊/疑似IFI且无需额外抗真菌药物)。在符合方案集和全分析集中评估米卡芬净对比标准治疗的非劣效性(10%的界值)。安全性评估包括不良事件以及肝肾功能检查。
全分析集包括344例患者(172例米卡芬净;172例标准治疗)。平均年龄为51.2岁;48.0%的患者终末期肝病模型评分≥20。在EOP时(平均治疗持续时间17天),符合方案集中米卡芬净的临床成功率为98.6%,标准治疗为99.3%(标准治疗-米卡芬净差值[95%置信区间],0.7%[-2.7%至4.4%]),全分析集中分别为96.5%和93.6%(-2.9%[-8.0%至1.9%])。米卡芬净和标准治疗的药物相关不良事件发生率分别为11.6%和16.3%,导致停药的病例分别为6.4%和11.6%。在EOP时,肝功能检查结果相似,但米卡芬净治疗的患者肌酐清除率高于标准治疗的患者。
在IFI高风险的肝移植患者中,米卡芬净作为抗真菌预防药物不劣于标准治疗。EOP时的不良事件谱和肝功能相似,尽管米卡芬净对肾功能的影响更好。
NCT01058174。