Gibney Geoffrey T, Kudchadkar Ragini R, DeConti Ronald C, Thebeau Melissa S, Czupryn Maria P, Tetteh Leticia, Eysmans Cabell, Richards Allison, Schell Michael J, Fisher Kate J, Horak Christine E, Inzunza H David, Yu Bin, Martinez Alberto J, Younos Ibrahim, Weber Jeffrey S
Department of Cutaneous Oncology and Comprehensive Melanoma Research Center, Moffitt Cancer Center, Tampa, Florida. Department of Oncologic Sciences, University of South Florida, Tampa, Florida.
Division of Oncology, Department of Medicine, Emory University School of Medicine, Atlanta, Georgia.
Clin Cancer Res. 2015 Feb 15;21(4):712-20. doi: 10.1158/1078-0432.CCR-14-2468. Epub 2014 Dec 18.
The anti-programmed death-1 (PD-1) antibody nivolumab (BMS-936558) has clinical activity in patients with metastatic melanoma. Nivolumab plus vaccine was investigated as adjuvant therapy in resected stage IIIC and IV melanoma patients.
HLA-A*0201 positive patients with HMB-45, NY-ESO-1, and/or MART-1 positive resected tumors received nivolumab (1 mg/kg, 3 mg/kg, or 10 mg/kg i.v.) with a multi-peptide vaccine (gp100, MART-1, and NY-ESO-1 with Montanide ISA 51 VG) every 2 weeks for 12 doses followed by nivolumab maintenance every 12 weeks for 8 doses. Primary objective was safety and determination of a maximum tolerated dose (MTD). Secondary objectives included relapse-free survival (RFS), overall survival (OS), and immunologic correlative studies.
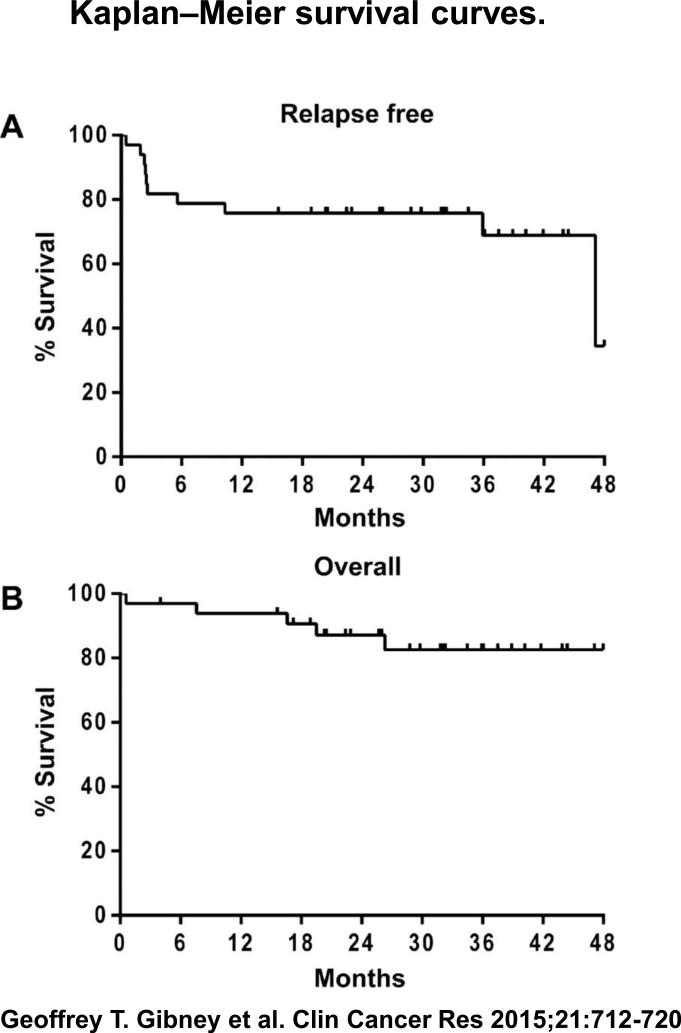
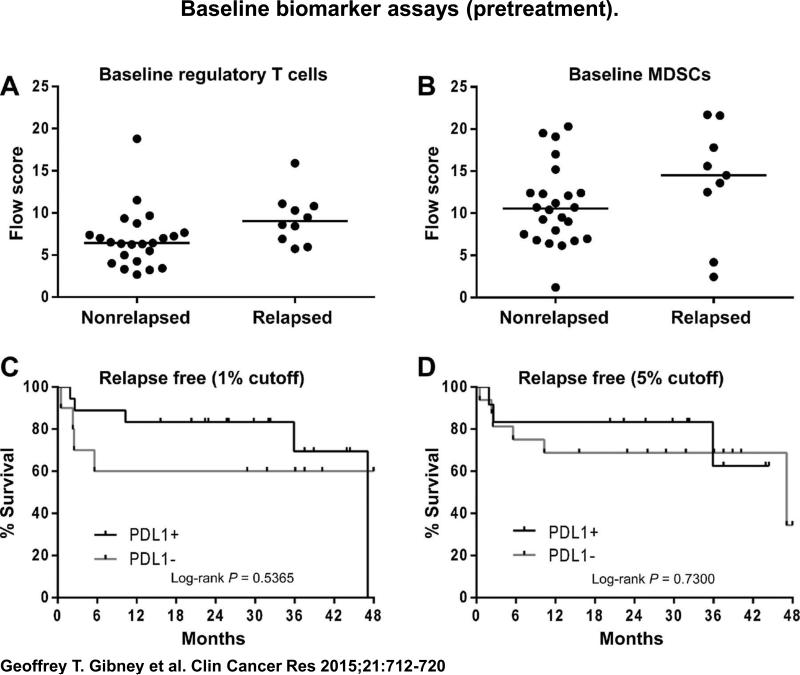
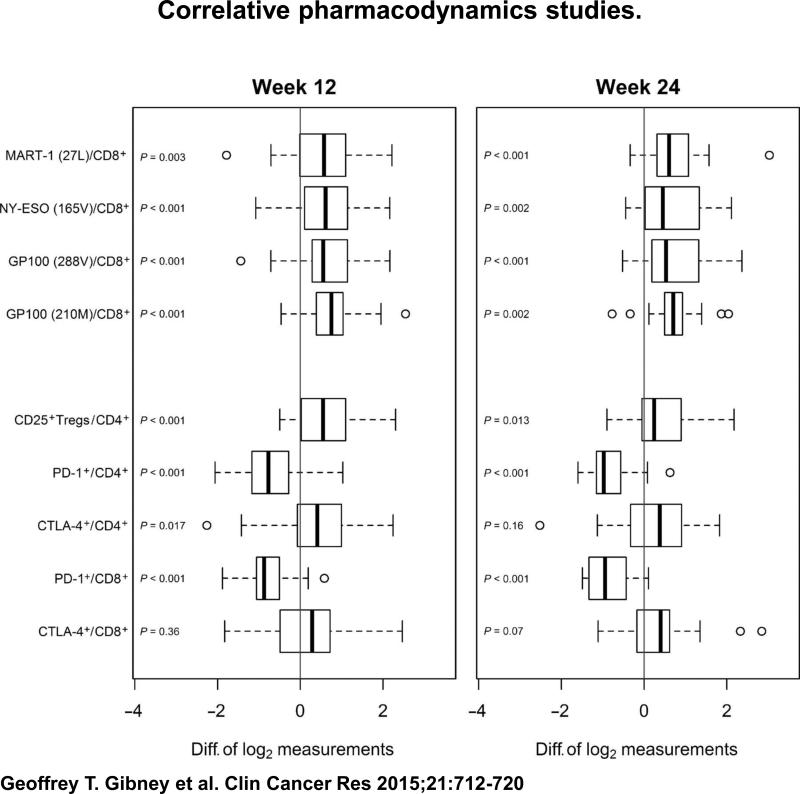
Thirty-three patients were enrolled. Median age was 47 years; 55% were male. Two patients had stage IIIC disease; 31 patients had stage IV disease. Median follow-up was 32.1 months. MTD was not reached. Most common related adverse events (>40%) were vaccine injection site reaction, fatigue, rash, pruritus, nausea, and arthralgias. Five related grade 3 adverse events [hypokalemia (1), rash (1), enteritis (1), and colitis (2)] were observed. Ten of 33 patients relapsed. Estimated median RFS was 47.1 months; median OS was not reached. Increases in CTLA-4(+)/CD4(+), CD25(+)Treg/CD4(+), and tetramer specific CD8(+) T-cell populations were observed with treatment (P < 0.05). Trends for lower baseline myeloid-derived suppressor cell and CD25(+)Treg/CD4(+) populations were seen in nonrelapsing patients; PD-L1 tumor status was not significantly associated with RFS.
Nivolumab with vaccine is well tolerated as adjuvant therapy and demonstrates immunologic activity with promising survival in high-risk resected melanoma, justifying further study.
抗程序性死亡-1(PD-1)抗体纳武单抗(BMS-936558)对转移性黑色素瘤患者具有临床活性。纳武单抗联合疫苗被作为辅助治疗用于已切除的IIIC期和IV期黑色素瘤患者。
HLA-A*0201阳性、肿瘤切除标本HMB-45、NY-ESO-1和/或MART-1阳性的患者接受纳武单抗(1mg/kg、3mg/kg或10mg/kg静脉注射)联合多肽疫苗(gp100、MART-1和NY-ESO-1与Montanide ISA 51 VG),每2周一次,共12剂,随后每12周一次纳武单抗维持治疗,共8剂。主要目标是安全性和确定最大耐受剂量(MTD)。次要目标包括无复发生存期(RFS)、总生存期(OS)和免疫相关性研究。
33例患者入组。中位年龄47岁;55%为男性。2例患者为IIIC期疾病;31例患者为IV期疾病。中位随访时间为32.1个月。未达到MTD。最常见的相关不良事件(>40%)为疫苗注射部位反应、疲劳、皮疹、瘙痒、恶心和关节痛。观察到5例相关的3级不良事件[低钾血症(1例)、皮疹(1例)、肠炎(1例)和结肠炎(2例)]。33例患者中有10例复发。估计中位RFS为47.1个月;未达到中位OS。治疗后观察到CTLA-4(+)/CD4(+)、CD25(+)调节性T细胞/CD4(+)和四聚体特异性CD8(+) T细胞群体增加(P<0.05)。在未复发患者中观察到基线髓源性抑制细胞和CD25(+)调节性T细胞/CD4(+)群体较低的趋势;PD-L1肿瘤状态与RFS无显著相关性。
纳武单抗联合疫苗作为辅助治疗耐受性良好,并在高危已切除黑色素瘤中显示出免疫活性和有前景的生存期,值得进一步研究。