Ram Nanik, Ali Syed Ahsan, Hussain Syed Zubair
Section of Endocrinology, Department of Medicine, The Aga Khan University Hospital, Stadium Road, Karachi 74800, Pakistan.
J Med Case Rep. 2014 Dec 19;8:445. doi: 10.1186/1752-1947-8-445.
Pituitary stalk interruption syndrome is a rare congenital abnormality of the pituitary that is responsible for anterior pituitary deficiency. It is characterized by a classic triad of interrupted pituitary stalk, absent or ectopic posterior pituitary, and anterior pituitary hypoplasia or aplasia. Clinical presentation varies according to age. In adults it presents as short stature and anterior pituitary deficiency. Without early diagnosis and treatment, mortality and morbidity in these patients is high. Early diagnosis and treatment of this rare disease can prevent permanent short statue of the patient. We report the first case of pituitary stalk interruption syndrome from Pakistan.
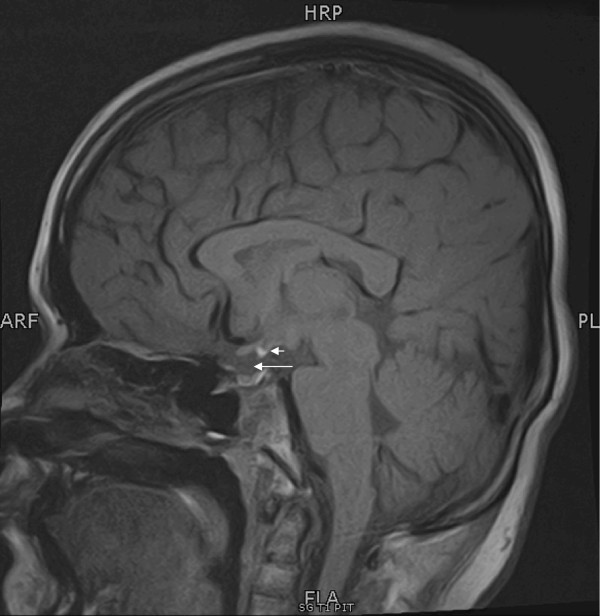
A 17-year-old Pakistani young man presented with short stature and underdeveloped secondary sexual characters. His siblings and parents were healthy, with normal height. An examination showed his blood pressure was 90/60 mmHg, and his height, weight, and body mass index were 142 cm, 34.5 kg, and 17.10 kg/m2, respectively. He had no hair growth on his face, axilla, or pubis. His testes were between 1 and 2 mL in size, with a 4 cm-at-stretch micropenis. His lab investigations showed that his thyroid stimulating hormone (TSH) was 8.58 uIU/mL (0.4 to 4.2), his free thyroid hormone level FT4 was 0.46 ng/dL (0.89 to 1.76), his prolactin was 21.1 ng/mL (3.0 to 14.7), and his baseline cortisol was 0.30 ug/dL (4.3 to 22.4). His cortisol level after 60 minutes of cosyntropin injection was 3.5 ug/dL (4.3 to 22.4), his insulin like growth factor IGF-1 was 31.56 ng/mL (247.3 to 481.7), his testosterone level was under 2.5 ng/dL (2 to 800), his follicle stimulating hormone FSH was 0.41 uIU/mL (0.0 to 10.0), and his leutinizing hormone LH was under 0.1 uIU/mL (1.2 to 7.8). His bone age was 10 years according to the Greulich and Pyle method, as shown by X-rays. The results from his pituitary magnetic resonance imaging scan were consistent with pituitary stalk interruption syndrome.
We describe a young man who presented with short stature and was found to have pituitary stalk interruption syndrome. Despite the fact that this is a rare disorder, it should always be kept in the differential diagnosis of a patient presenting with short stature. Patients with this disease have an excellent opportunity to reach normal height if they present before the joining of epiphyses.
垂体柄中断综合征是一种罕见的先天性垂体异常疾病,可导致腺垂体功能减退。其特征为垂体柄中断、垂体后叶缺如或异位以及腺垂体发育不全或不发育这一典型三联征。临床表现因年龄而异。在成年人中,表现为身材矮小和腺垂体功能减退。若不及早诊断和治疗,这些患者的死亡率和发病率会很高。对这种罕见疾病的早诊断和治疗可防止患者永久性身材矮小。我们报告了巴基斯坦首例垂体柄中断综合征病例。
一名17岁的巴基斯坦青年男性,因身材矮小及第二性征发育不全前来就诊。他的兄弟姐妹及父母均健康,身高正常。检查显示其血压为90/60 mmHg,身高、体重及体重指数分别为142 cm、34.5 kg和17.10 kg/m²。他面部、腋窝及耻骨部位均无毛发。其睾丸大小在1至2 mL之间,阴茎牵拉长度为4 cm。实验室检查显示,他的促甲状腺激素(TSH)为8.58 uIU/mL(0.4至4.2),游离甲状腺激素水平FT4为0.46 ng/dL(0.89至1.76),催乳素为21.1 ng/mL(3.0至14.7),基础皮质醇为0.30 ug/dL(4.3至22.4)。注射促肾上腺皮质激素60分钟后的皮质醇水平为3.5 ug/dL(4.3至22.4),胰岛素样生长因子IGF-1为31.56 ng/mL(247.3至481.7),睾酮水平低于2.5 ng/dL(2至800),促卵泡生成素FSH为0.41 uIU/mL(0.0至10.0),促黄体生成素LH低于0.1 uIU/mL(1.2至7.8)。X线检查显示,根据格-派方法,其骨龄为10岁。垂体磁共振成像扫描结果与垂体柄中断综合征相符。
我们描述了一名身材矮小且被诊断为垂体柄中断综合征的青年男性。尽管这是一种罕见疾病,但对于身材矮小的患者,在鉴别诊断时应始终考虑到该病。如果骨骺尚未融合时就发现患有此病,患者有机会达到正常身高。