Hao Zilong, Yang Chunsong, Liu Ming, Wu Bo
From the Stroke Clinical Research Unit, Department of Neurology, West China Hospital, Sichuan University, No 37, Guo Xue Xiang, Chengdu 610041, China (ZH, ML, BW); Department of Pharmacy, Evidence-Based Pharmacy Center, West China Second Hospital, Key Laboratory of Birth Defects and Related Diseases of Women and Children, Sichuan University, Chengdu, 610041 China (CY).
Medicine (Baltimore). 2014 Dec;93(28):e286. doi: 10.1097/MD.0000000000000286.
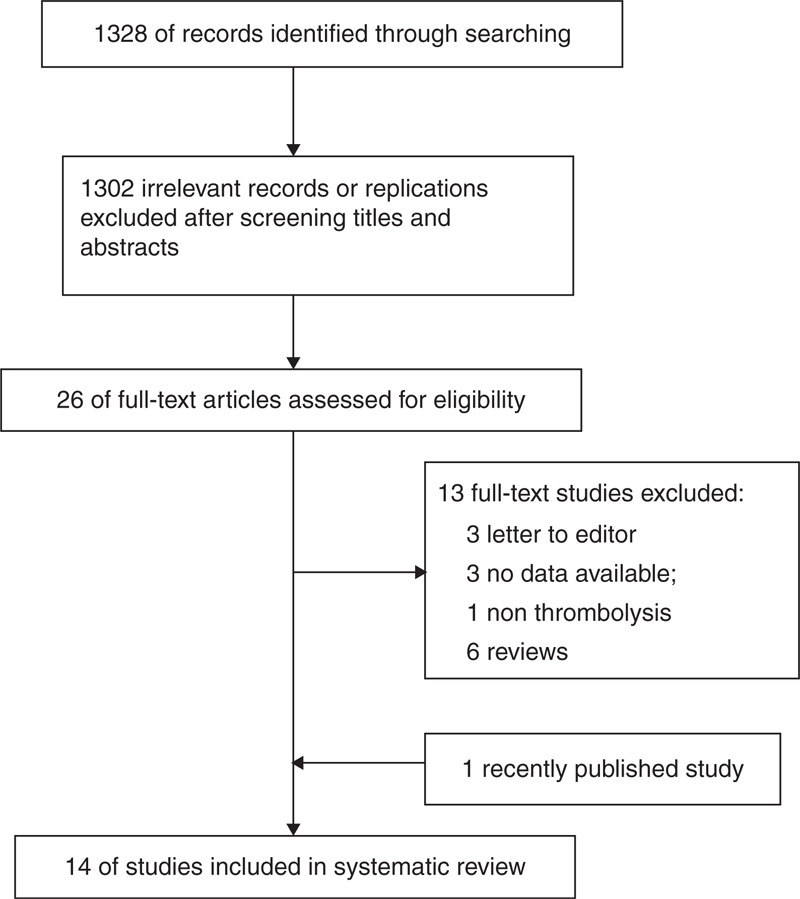
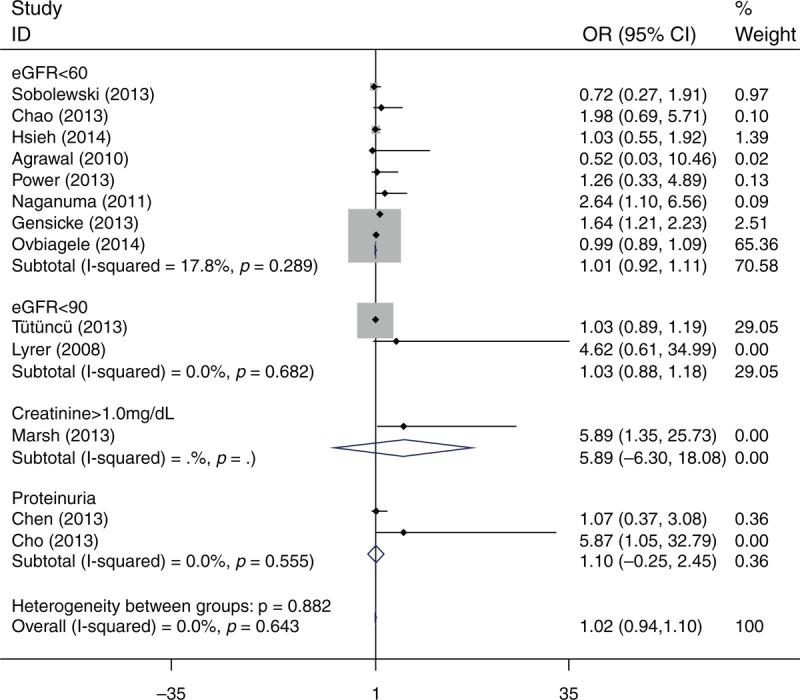
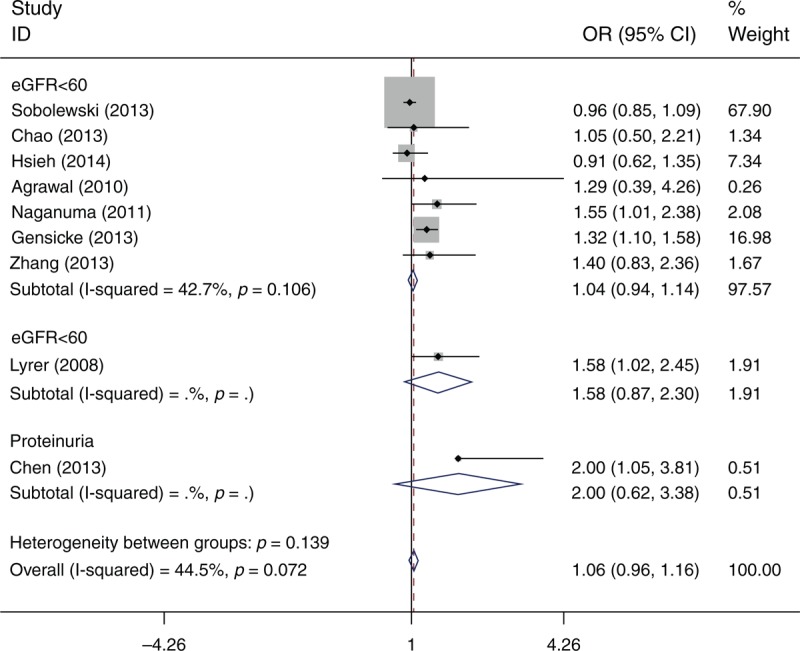
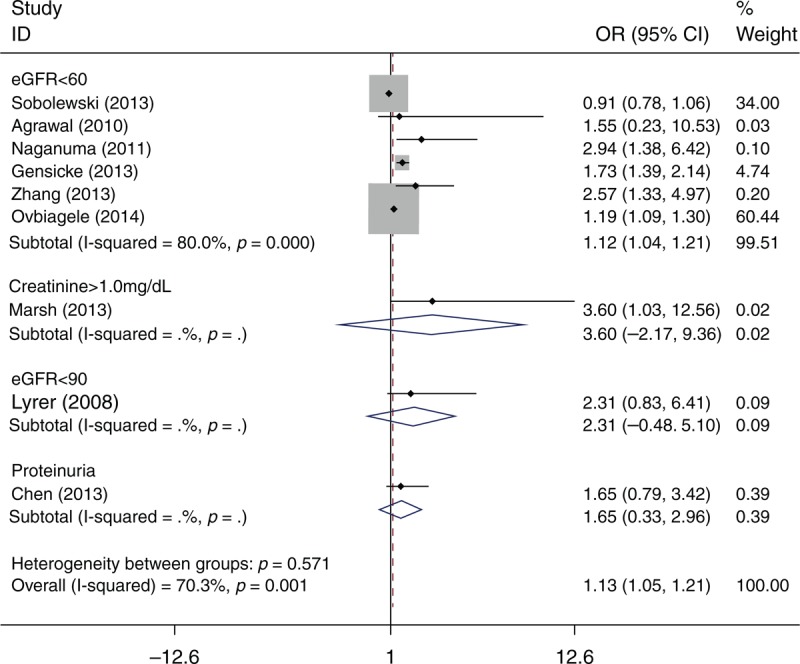
Renal dysfunction is a prevalent comorbidity in acute ischemic stroke patients requiring thrombolytic therapy. However, the effect of renal dysfunction on the clinical outcome of this population remains controversial. This study aimed to evaluate the safety and effectiveness of thrombolytic therapy in acute stroke patients with renal dysfunction using a meta-analysis. We systematically searched PubMed and EMBASE for studies that evaluated the relationship between renal dysfunction and intravenous tissue plasminogen activator (tPA) in patients with acute ischemic stroke. Poor outcome (modified Rankin Scale≥2), mortality, and symptomatic intracranial hemorrhage (ICH) and any ICH were analyzed. Fourteen studies were included (N=53,553 patients). The mean age ranged from 66 to 75 years. The proportion of male participants was 49% to 74%. The proportion of renal dysfunction varied from 21.9% to 83% according to different definitions. Based on 9 studies with a total of 7796 patients, the meta-analysis did not identify a significant difference in the odds of poor outcome (odds ratio [OR]=1.06; 95% confidence interval [CI]: 0.96-1.16; I=44.5) between patients with renal dysfunction and those without renal dysfunction. Patients with renal dysfunction were more likely to die after intravenous thrombolysis (OR=1.13; 95% CI: 1.05-1.21; I=70.3). No association was observed between symptomatic ICH (OR=1.02; 95% CI: 0.94-1.10; I=0) and any ICH (OR=1.07; 95% CI: 0.96-1.18; I=25.8). Renal dysfunction does not increase the risk of poor outcome and ICH after stroke thrombolysis. Renal dysfunction should not be a contraindication for administration of intravenous thrombolysis to eligible patients.
肾功能不全是需要溶栓治疗的急性缺血性卒中患者中常见的合并症。然而,肾功能不全对该人群临床结局的影响仍存在争议。本研究旨在通过荟萃分析评估肾功能不全的急性卒中患者溶栓治疗的安全性和有效性。我们系统检索了PubMed和EMBASE,以查找评估急性缺血性卒中患者肾功能不全与静脉注射组织型纤溶酶原激活剂(tPA)之间关系的研究。分析了不良结局(改良Rankin量表≥2)、死亡率、症状性颅内出血(ICH)和任何颅内出血情况。纳入了14项研究(N = 53553例患者)。平均年龄在66至75岁之间。男性参与者比例为49%至74%。根据不同定义,肾功能不全的比例在21.9%至83%之间。基于9项共7796例患者的研究,荟萃分析未发现肾功能不全患者与无肾功能不全患者在不良结局几率方面存在显著差异(优势比[OR]=1.06;95%置信区间[CI]:0.96 - 1.16;I² = 44.5)。肾功能不全患者静脉溶栓后死亡可能性更大(OR = 1.13;95% CI:1.05 - 1.21;I² = 70.3)。未观察到症状性ICH(OR = 1.02;95% CI:0.94 - 1.10;I² = 0)和任何颅内出血(OR = 1.07;95% CI:0.96 - 1.18;I² = 25.8)之间存在关联。肾功能不全不会增加卒中溶栓后不良结局和颅内出血的风险。肾功能不全不应成为符合条件患者静脉溶栓给药的禁忌证。