Kollmer Jennifer, Hund Ernst, Hornung Benjamin, Hegenbart Ute, Schönland Stefan O, Kimmich Christoph, Kristen Arnt V, Purrucker Jan, Röcken Christoph, Heiland Sabine, Bendszus Martin, Pham Mirko
1 Department of Neuroradiology, University of Heidelberg, Heidelberg, Germany 2 Amyloidosis Centre Heidelberg, University of Heidelberg, Heidelberg, Germany
2 Amyloidosis Centre Heidelberg, University of Heidelberg, Heidelberg, Germany 3 Department of Neurology, University of Heidelberg, Heidelberg, Germany.
Brain. 2015 Mar;138(Pt 3):549-62. doi: 10.1093/brain/awu344. Epub 2014 Dec 18.
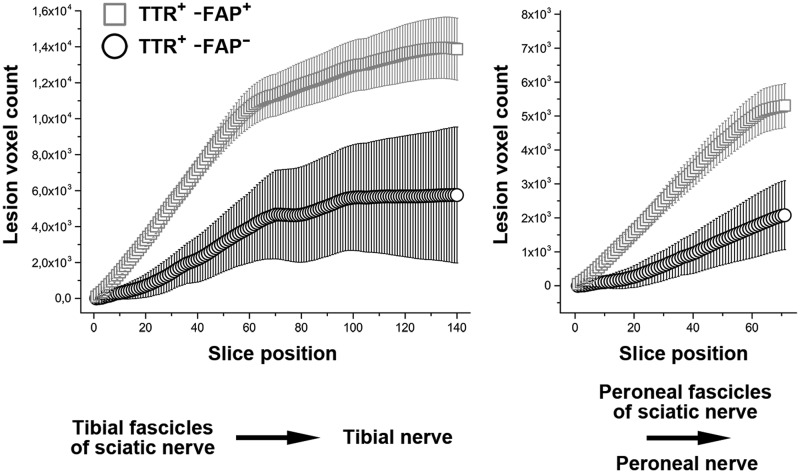
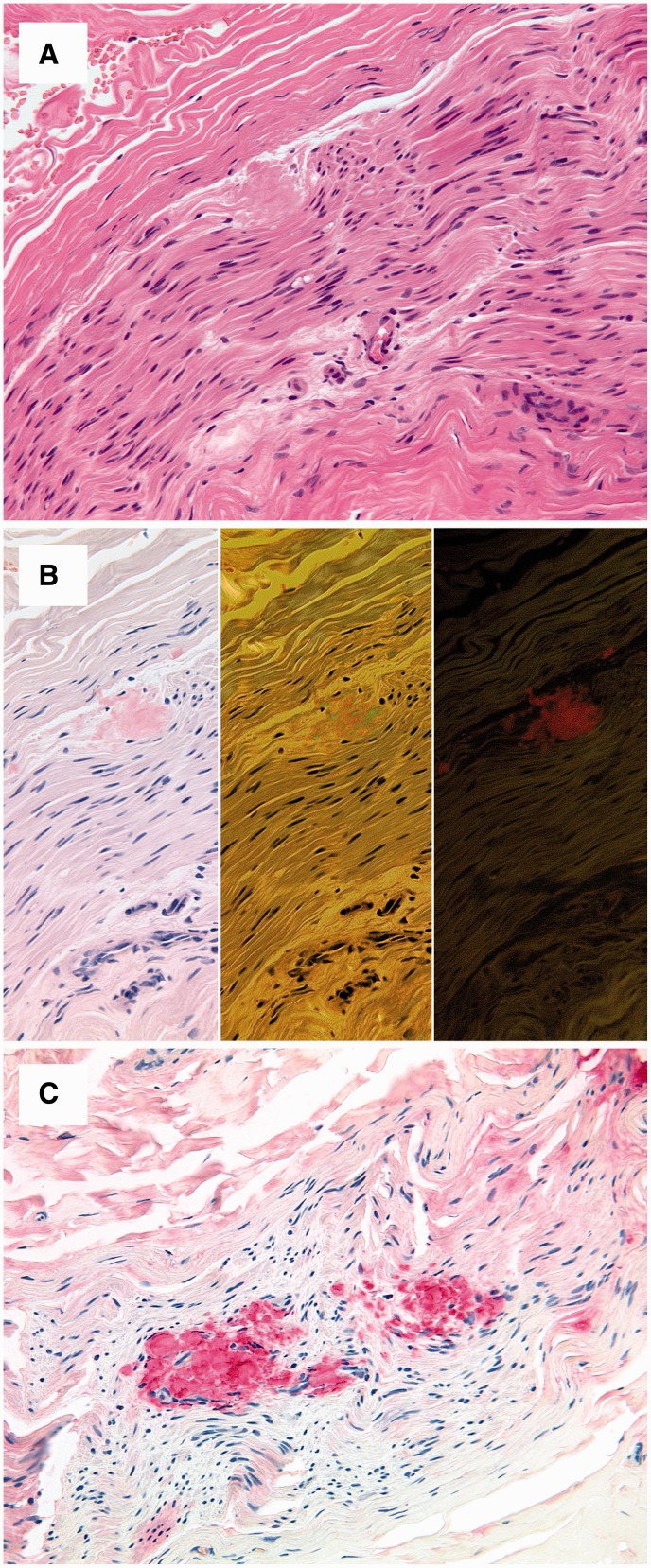
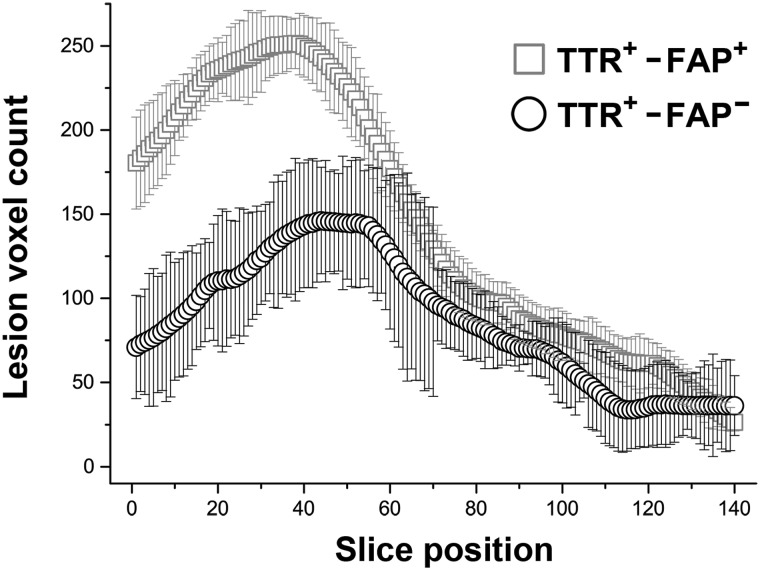
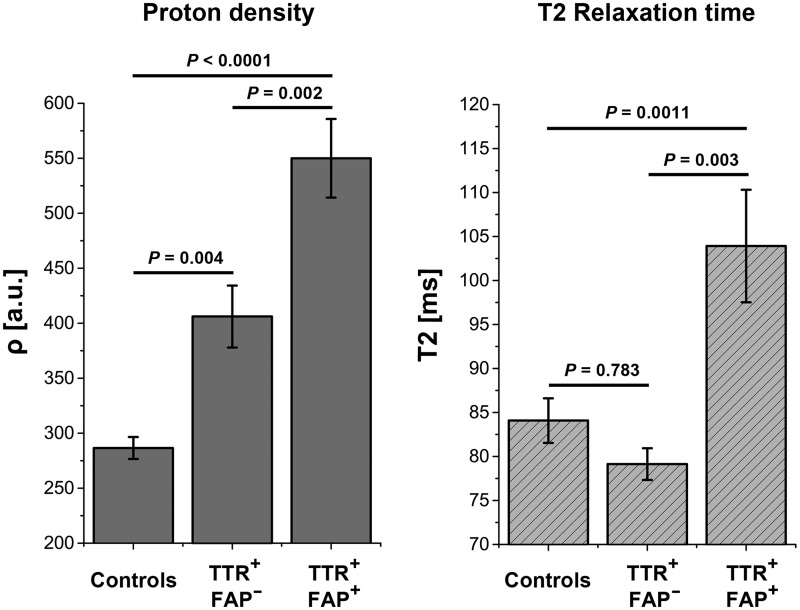
Transthyretin familial amyloid polyneuropathy is a rare, autosomal-dominant inherited multisystem disorder usually manifesting with a rapidly progressive, axonal, distally-symmetric polyneuropathy. The detection of nerve injury by nerve conduction studies is limited, due to preferential involvement of small-fibres in early stages. We investigated whether lower limb nerve-injury can be detected, localized and quantified in vivo by high-resolution magnetic resonance neurography. We prospectively included 20 patients (12 male and eight female patients, mean age 47.9 years, range 26-66) with confirmed mutation in the transthyretin gene: 13 with symptomatic polyneuropathy and seven asymptomatic gene carriers. A large age- and sex-matched cohort of healthy volunteers served as controls (20 male and 20 female, mean age 48.1 years, range 30-73). All patients received detailed neurological and electrophysiological examinations and were scored using the Neuropathy Impairment Score-Lower Limbs, Neuropathy Deficit and Neuropathy Symptom Score. Magnetic resonance neurography (3 T) was performed with large longitudinal coverage from proximal thigh to ankle-level and separately for each leg (140 axial slices/leg) by using axial T2-weighted (repetition time/echo time = 5970/55 ms) and dual echo (repetition time 5210 ms, echo times 12 and 73 ms) turbo spin echo 2D sequences with spectral fat saturation. A 3D T2-weighted inversion-recovery sequence (repetition time/echo time 3000/202 ms) was acquired for imaging of the spinal nerves and lumbar plexus (50 axial slice reformations). Precise manual segmentation of the spinal/sciatic/tibial/common peroneal nerves was performed on each slice. Histogram-based normalization of nerve-voxel signal intensities was performed using the age- and sex-matched control group as normative reference. Nerve-voxels were subsequently classified as lesion-voxels if a threshold of >1.2 (normalized signal-intensity) was exceeded. At distal thigh level, where a predominant nerve-lesion-voxel burden was observed, signal quantification was performed by calculating proton spin density and T2-relaxation time as microstructural markers of nerve tissue integrity. The total number of nerve-lesion voxels (cumulated from proximal-to-distal) was significantly higher in symptomatic patients (20 405 ± 1586) versus asymptomatic gene carriers (12 294 ± 3199; P = 0.036) and versus controls (6536 ± 467; P < 0.0001). It was also higher in asymptomatic carriers compared to controls (P = 0.043). The number of nerve-lesion voxels was significantly higher at thigh level compared to more distal levels (lower leg/ankle) of the lower extremities (f-value = 279.22, P < 0.0001). Further signal-quantification at this proximal site (thigh level) revealed a significant increase of proton-density (P < 0.0001) and T2-relaxation-time (P = 0.0011) in symptomatic patients, whereas asymptomatic gene-carriers presented with a significant increase of proton-density only. Lower limb nerve injury could be detected and quantified in vivo on microstructural level by magnetic resonance neurography in symptomatic familial amyloid polyneuropathy, and also in yet asymptomatic gene carriers, in whom imaging detection precedes clinical and electrophysiological manifestation. Although symptoms start and prevail distally, the focus of predominant nerve injury and injury progression was found proximally at thigh level with strong and unambiguous lesion-contrast. Imaging of proximal nerve lesions, which are difficult to detect by nerve conduction studies, may have future implications also for other distally-symmetric polyneuropathies.
转甲状腺素蛋白家族性淀粉样多神经病是一种罕见的常染色体显性遗传多系统疾病,通常表现为快速进展的轴索性、远端对称性多神经病。由于早期阶段小纤维优先受累,神经传导研究对神经损伤的检测有限。我们研究了高分辨率磁共振神经成像是否能够在体内检测、定位和量化下肢神经损伤。我们前瞻性纳入了20例转甲状腺素蛋白基因确诊突变的患者(12例男性和8例女性患者,平均年龄47.9岁,范围26 - 66岁):13例有症状性多神经病患者和7例无症状基因携带者。一大组年龄和性别匹配的健康志愿者作为对照(20例男性和20例女性,平均年龄48.1岁,范围30 - 73岁)。所有患者均接受了详细的神经学和电生理检查,并使用下肢神经病变评分、神经病变缺损和神经病变症状评分进行评分。采用3T磁共振神经成像,从大腿近端至踝关节水平进行大的纵向覆盖,每条腿分别成像(每条腿140个轴位切片),使用轴向T2加权(重复时间/回波时间 = 5970/55 ms)和双回波(重复时间5210 ms,回波时间12和73 ms)涡轮自旋回波2D序列并结合频谱脂肪饱和技术。采集一个3D T2加权反转恢复序列(重复时间/回波时间3000/202 ms)用于脊髓神经和腰丛成像(50个轴位切片重组)。在每个切片上对脊髓/坐骨神经/胫神经/腓总神经进行精确的手动分割。使用年龄和性别匹配的对照组作为标准参考,对神经体素信号强度进行基于直方图的归一化。如果超过>1.2(归一化信号强度)的阈值,则将神经体素随后分类为病变体素。在大腿远端水平观察到主要的神经病变体素负荷,通过计算质子自旋密度和T2弛豫时间作为神经组织完整性的微观结构标志物进行信号量化。有症状患者(20405±1586)的神经病变体素总数(从近端到远端累计)显著高于无症状基因携带者(12294±3199;P = 0.036)和对照组(6536±467;P < 0.0001)。与对照组相比,无症状携带者的神经病变体素总数也更高(P = 0.043)。与下肢更远端水平(小腿/踝关节)相比,大腿水平的神经病变体素数量显著更高(F值 = 279.22,P < 0.0001)。在这个近端部位(大腿水平)进一步的信号量化显示,有症状患者的质子密度(P < 0.0001)和T2弛豫时间(P = 0.0011)显著增加,而无症状基因携带者仅质子密度显著增加。磁共振神经成像能够在微观结构水平上在体内检测和量化有症状的家族性淀粉样多神经病患者以及尚未出现症状的基因携带者的下肢神经损伤,在这些患者中,成像检测先于临床和电生理表现。尽管症状始于并主要出现在远端,但主要神经损伤和损伤进展的焦点在近端大腿水平被发现,具有强烈且明确的病变对比。对于神经传导研究难以检测的近端神经病变进行成像,可能对其他远端对称性多神经病也具有未来意义。