Burman Robert Anders, Zakariassen Erik, Hunskaar Steinar
National Centre for Emergency Primary Health Care, Uni Research Health, Kalfarveien 31, 5018, Bergen, Norway.
Department of Global Public Health and Primary Care, University of Bergen, Post box 7804, 5020, Bergen, Norway.
BMC Fam Pract. 2014 Dec 21;15:207. doi: 10.1186/s12875-014-0207-4.
Acute chest pain constitutes a considerable diagnostic challenge outside hospitals. This will often lead to uncertainty in choosing the right management, and the physicians' approach may be influenced by their knowledge of diagnostic measures and their tolerance of risk. The aim of this study was to investigate primary care physicians' diagnostic approach, tolerance of risk and attitudes to hospital admission in patients with acute chest pain out-of-hours in Norwegian primary care.
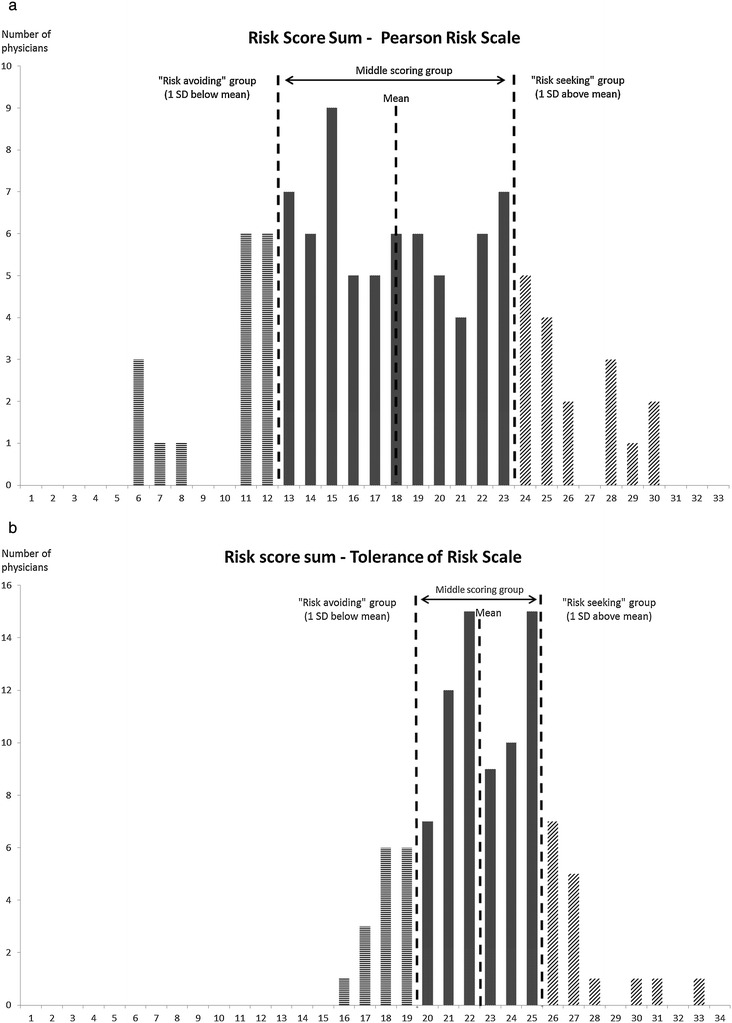
Data were registered prospectively from four Norwegian casualty clinics. Data from structured telephone interviews with 100 physicians shortly after a consultation with a patient presenting at the casualty clinic with "chest pain" were analysed. Tolerance of risk was measured by the Pearson Risk Scale and the Tolerance of Risk Scale, the latter developed for this study.
"Patient history and symptoms" was considered the most important, and "negative ECG" and "effect of sublingual nitroglycerine" the least important aspects in the diagnostic approach. There were no significant differences in length of experience or gender when testing "risk avoiders" against the rest. Almost all physicians felt that their risk assessment out-of-hours was reasonably good, and felt reasonably safe, but only 50% agreed with the statement "I don't worry about my decisions after I've made them". Concerning chest pain patients only, 51% of the physicians were worried about complaints being made about them, 75% agreed that admitting someone to hospital put patients in danger of being "over-tested", and 51% were more likely to admit the patient if the patient herself wanted to be admitted.
Physicians working out-of-hours showed considerable differences in their diagnostic approach, and not all physicians diagnose patients with chest pain according to current guidelines and evidence. Continuous medical education must focus on the diagnostic approach in patients with chest pain in primary care and empowerment of physicians through training and emphasis on risk assessment and "tolerance of risk".
急性胸痛在院外构成了相当大的诊断挑战。这常常会导致在选择正确治疗方案时产生不确定性,医生的处理方式可能会受到其对诊断措施的了解以及对风险的容忍度的影响。本研究的目的是调查挪威初级医疗中,初级保健医生在非工作时间对急性胸痛患者的诊断方法、风险容忍度以及对住院治疗的态度。
前瞻性地记录了来自挪威四家急诊诊所的数据。对在急诊诊所与“胸痛”患者会诊后不久接受结构化电话访谈的100名医生的数据进行了分析。风险容忍度通过皮尔逊风险量表和为本研究开发的风险容忍量表进行测量。
在诊断方法中,“患者病史和症状”被认为是最重要的,而“心电图阴性”和“舌下硝酸甘油的效果”被认为是最不重要的方面。在将“风险规避者”与其他医生进行比较时,经验长度或性别方面没有显著差异。几乎所有医生都认为他们在非工作时间的风险评估相当不错,并且感觉相当安全,但只有50%的医生同意“做出决定后我不担心自己的决定”这一说法。仅就胸痛患者而言,51%的医生担心会收到针对他们的投诉,75%的医生同意将患者收治入院会使患者面临“过度检查”的风险,并且51%的医生表示如果患者自己希望入院,他们更有可能收治该患者。
非工作时间工作的医生在诊断方法上存在相当大的差异,并非所有医生都根据当前指南和证据对胸痛患者进行诊断。继续医学教育必须侧重于初级医疗中胸痛患者的诊断方法,以及通过培训和强调风险评估及“风险容忍度”来增强医生的能力。