Simon Marcel, Braune Stephan, Frings Daniel, Wiontzek Ann-Kathrin, Klose Hans, Kluge Stefan
Department of Intensive Care Medicine, University Medical Centre Hamburg-Eppendorf, Martinistr. 52, 20246, Hamburg, Germany.
Department of Respiratory Medicine, University Medical Centre Hamburg-Eppendorf, Martinistr. 52, 20246, Hamburg, Germany.
Crit Care. 2014 Dec 22;18(6):712. doi: 10.1186/s13054-014-0712-9.
Critically ill patients with respiratory failure undergoing bronchoscopy have an increased risk of hypoxaemia-related complications. Previous studies have shown that in awake, hypoxaemic patients non-invasive ventilation (NIV) is helpful in preventing gas exchange deterioration during bronchoscopy. An alternative and increasingly used means of oxygen delivery is its application via high-flow nasal cannula (HFNC). This study was conducted to compare HFNC with NIV in patients with acute hypoxaemic respiratory failure undergoing flexible bronchoscopy.
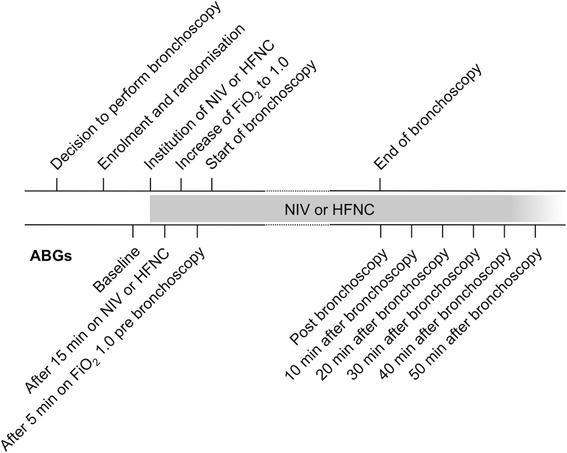
Prospective randomised trial randomising 40 critically ill patients with hypoxaemic respiratory failure to receive either NIV or HFNC during bronchoscopy in the intensive care unit.
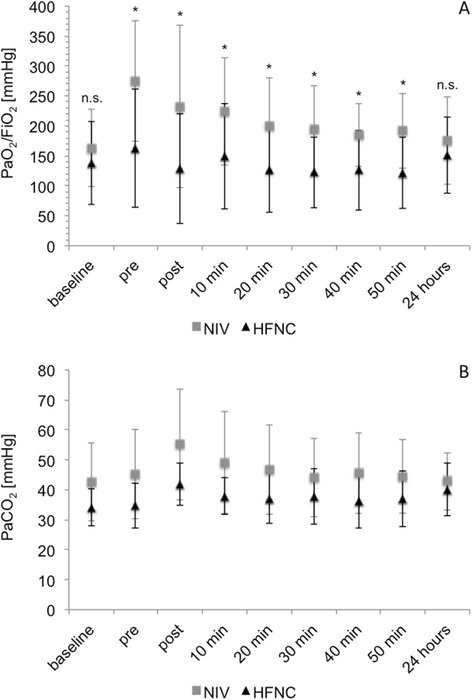
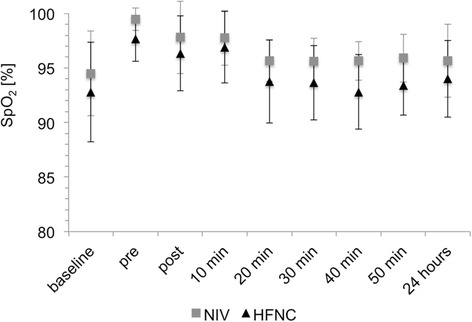
After the initiation of NIV and HFNC, oxygen levels were significantly higher in the NIV group compared to the HFNC group. Two patients were unable to proceed to bronchoscopy after the institution of HFNC due to progressive hypoxaemia. During bronchoscopy, one patient on HFNC deteriorated due to intravenous sedation requiring non-invasive ventilatory support. Bronchoscopy was well tolerated in all other patients. There were no significant differences between the two groups regarding heart rate, mean arterial pressure and respiratory rate. Three patients in the NIV group and one patient in the HFNC group were intubated within 24 hours after the end of bronchoscopy (P = 0.29).
The application of NIV was superior to HFNC with regard to oxygenation before, during and after bronchoscopy in patients with moderate to severe hypoxaemia. In patients with stable oxygenation under HFNC, subsequent bronchoscopy was well tolerated.
ClinicalTrials.gov NCT01870765. Registered 30 May 2013.
接受支气管镜检查的呼吸衰竭重症患者发生低氧血症相关并发症的风险增加。既往研究表明,对于清醒的低氧血症患者,无创通气(NIV)有助于预防支气管镜检查期间气体交换恶化。一种越来越常用的氧气输送方式是通过高流量鼻导管(HFNC)供氧。本研究旨在比较HFNC与NIV在接受柔性支气管镜检查的急性低氧血症呼吸衰竭患者中的应用效果。
前瞻性随机试验,将40例低氧血症呼吸衰竭重症患者随机分为两组,分别在重症监护病房进行支气管镜检查时接受NIV或HFNC。
开始NIV和HFNC后,NIV组的氧水平显著高于HFNC组。2例患者在采用HFNC后因进行性低氧血症而无法进行支气管镜检查。在支气管镜检查期间,1例接受HFNC的患者因静脉镇静需要无创通气支持而病情恶化。所有其他患者对支气管镜检查耐受性良好。两组在心率、平均动脉压和呼吸频率方面无显著差异。支气管镜检查结束后24小时内,NIV组有3例患者和HFNC组有1例患者进行了气管插管(P = 0.29)。
在中重度低氧血症患者中,支气管镜检查前、检查期间和检查后,NIV在氧合方面优于HFNC。在HFNC下氧合稳定的患者中,后续支气管镜检查耐受性良好。
ClinicalTrials.gov NCT01870765。2013年5月30日注册。