Chen Yunching, Ramjiawan Rakesh R, Reiberger Thomas, Ng Mei R, Hato Tai, Huang Yuhui, Ochiai Hiroki, Kitahara Shuji, Unan Elizabeth C, Reddy Tejaswini P, Fan Christopher, Huang Peigen, Bardeesy Nabeel, Zhu Andrew X, Jain Rakesh K, Duda Dan G
E.L. Steele Laboratory for Tumor Biology, Department of Radiation Oncology, Massachusetts General Hospital Cancer Center, Harvard Medical School, Boston, MA; Institute of Biomedical Engineering, National Tsing Hua University, Hsinchu, Taiwan.
Hepatology. 2015 May;61(5):1591-602. doi: 10.1002/hep.27665. Epub 2015 Mar 20.
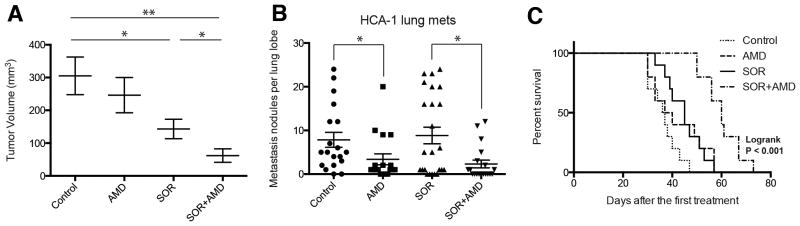
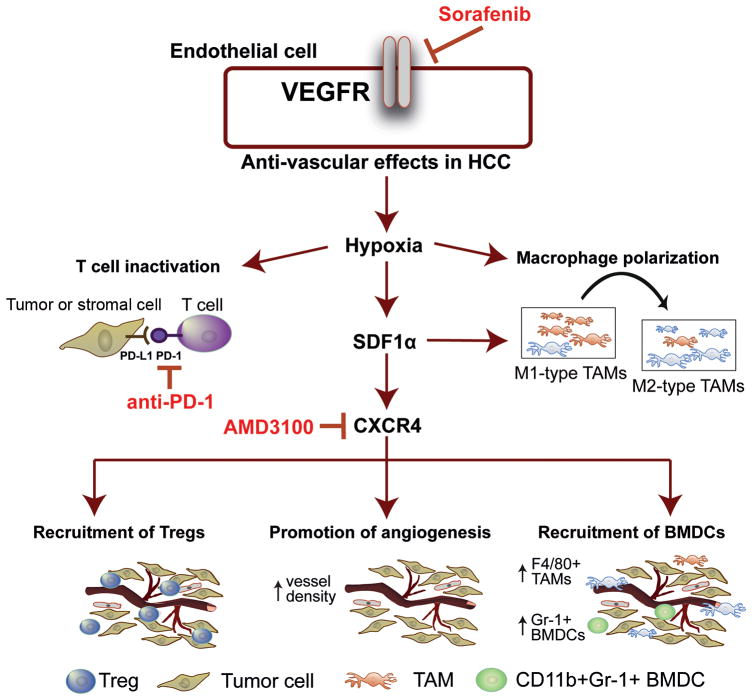
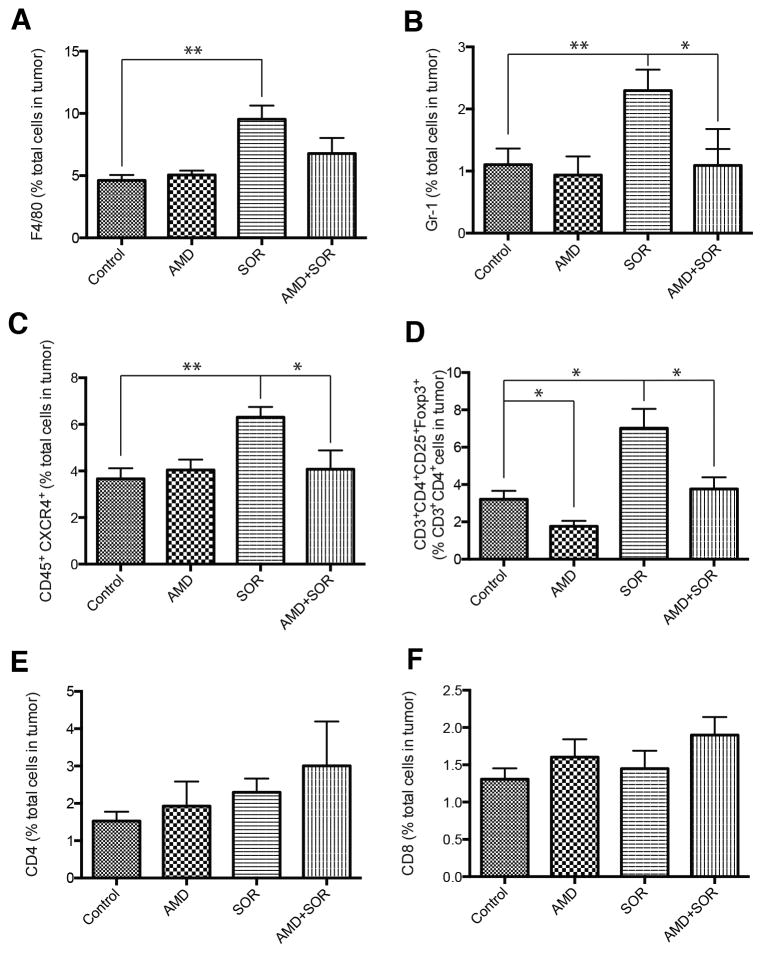
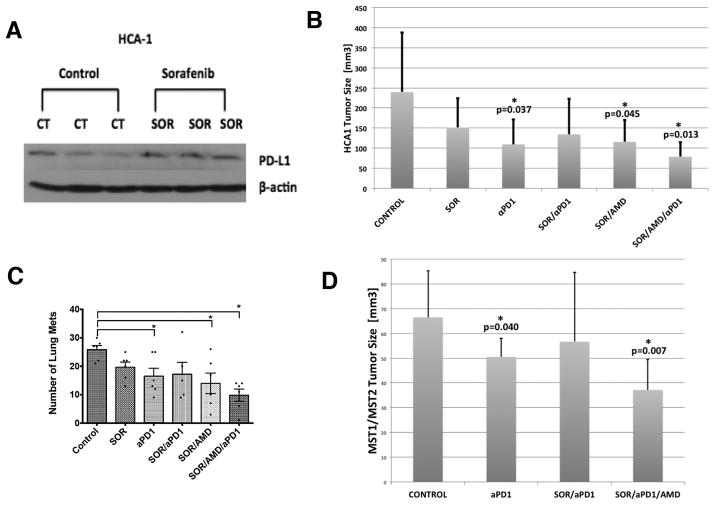
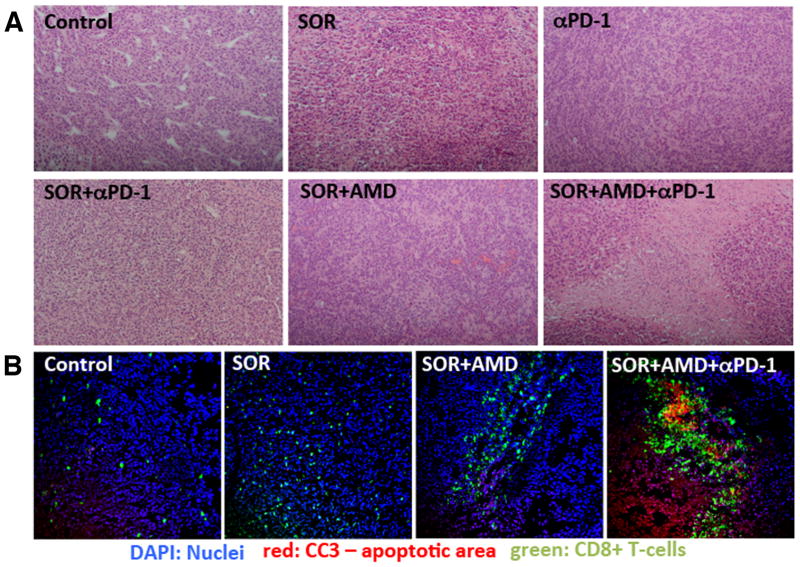
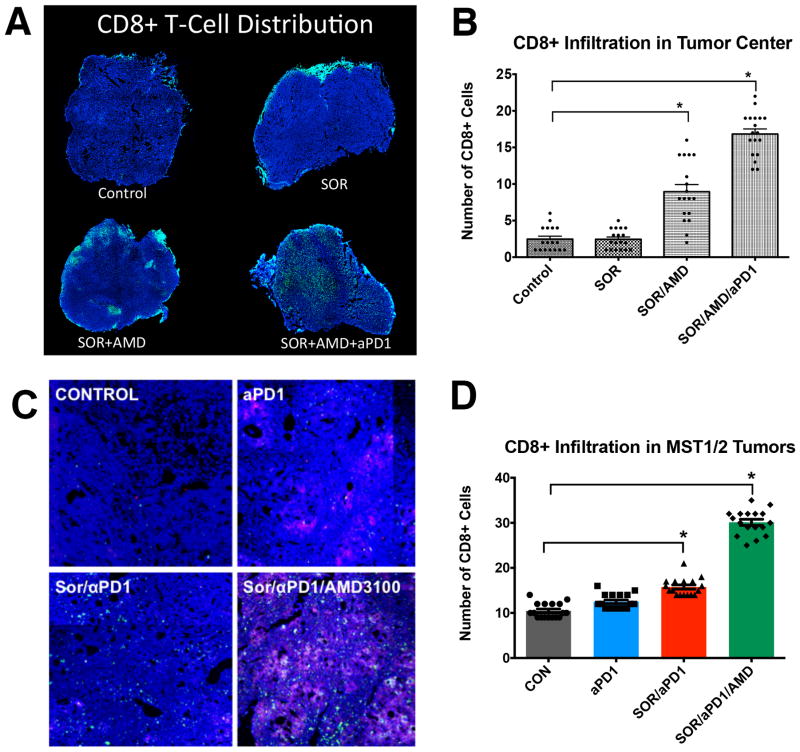
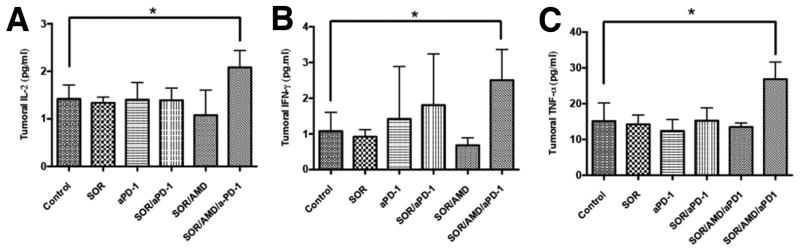
Sorafenib, a broad tyrosine kinase inhibitor, is the only approved systemic therapy for advanced hepatocellular carcinoma (HCC) but provides limited survival benefits. Recently, immunotherapy has emerged as a promising treatment strategy, but its role remains unclear in HCCs, which are associated with decreased cytotoxic CD8(+) T-lymphocyte infiltration in both murine and human tumors. Moreover, in mouse models after sorafenib treatment intratumoral hypoxia is increased and may fuel evasive resistance. Using orthotopic HCC models, we now show that increased hypoxia after sorafenib treatment promotes immunosuppression, characterized by increased intratumoral expression of the immune checkpoint inhibitor programmed death ligand-1 and accumulation of T-regulatory cells and M2-type macrophages. We also show that the recruitment of immunosuppressive cells is mediated in part by hypoxia-induced up-regulation of stromal cell-derived 1 alpha. Inhibition of the stromal cell-derived 1 alpha receptor (C-X-C receptor type 4 or CXCR4) using AMD3100 prevented the polarization toward an immunosuppressive microenvironment after sorafenib treatment, inhibited tumor growth, reduced lung metastasis, and improved survival. However, the combination of AMD3100 and sorafenib did not significantly change cytotoxic CD8(+) T-lymphocyte infiltration into HCC tumors and did not modify their activation status. In separate experiments, antibody blockade of the programmed death ligand-1 receptor programmed death receptor-1 (PD-1) showed antitumor effects in treatment-naive tumors in orthotopic (grafted and genetically engineered) models of HCC. However, anti-PD-1 antibody treatment had additional antitumor activity only when combined with sorafenib and AMD3100 and not when combined with sorafenib alone.
Anti-PD-1 treatment can boost antitumor immune responses in HCC models; when used in combination with sorafenib, anti-PD-1 immunotherapy shows efficacy only with concomitant targeting of the hypoxic and immunosuppressive microenvironment with agents such as CXCR4 inhibitors.
索拉非尼是一种广泛的酪氨酸激酶抑制剂,是唯一被批准用于晚期肝细胞癌(HCC)的全身治疗药物,但生存获益有限。最近,免疫疗法已成为一种有前景的治疗策略,但其在HCC中的作用仍不明确,HCC在小鼠和人类肿瘤中均与细胞毒性CD8(+) T淋巴细胞浸润减少有关。此外,在索拉非尼治疗后的小鼠模型中,肿瘤内缺氧增加,可能助长逃避性耐药。利用原位HCC模型,我们现在表明,索拉非尼治疗后缺氧增加会促进免疫抑制,其特征是肿瘤内免疫检查点抑制剂程序性死亡配体-1表达增加以及T调节细胞和M2型巨噬细胞积聚。我们还表明,免疫抑制细胞的募集部分由缺氧诱导的基质细胞衍生因子1α上调介导。使用AMD3100抑制基质细胞衍生因子1α受体(C-X-C受体4型或CXCR4)可防止索拉非尼治疗后向免疫抑制微环境极化,抑制肿瘤生长,减少肺转移,并改善生存。然而,AMD3100与索拉非尼联合使用并未显著改变细胞毒性CD8(+) T淋巴细胞浸润到HCC肿瘤中的情况,也未改变其激活状态。在单独的实验中,程序性死亡配体-1受体程序性死亡受体-1(PD-1)的抗体阻断在原位(移植和基因工程)HCC模型的未治疗肿瘤中显示出抗肿瘤作用。然而,抗PD-1抗体治疗仅在与索拉非尼和AMD3100联合使用时具有额外的抗肿瘤活性,而与单独的索拉非尼联合使用时则没有。
抗PD-1治疗可增强HCC模型中的抗肿瘤免疫反应;当与索拉非尼联合使用时,抗PD-1免疫疗法仅在与CXCR4抑制剂等药物同时靶向缺氧和免疫抑制微环境时才显示出疗效。