Zafar Hanna M, Harhay Michael O, Yang Jianing, Armstron Katrina
Department of Radiology Hospital of the University of Pennsylvania 3400 Spruce Street Philadelphia, PA 19104 ; Leonard Davis Institute of Health Economics University of Pennsylvania Colonial Penn Center, 3641 Locust Walk Philadelphia, PA 19104-6218 Philadelphia, United States.
Department of Medicine Hospital of the University of Pennsylvania 3400 Spruce Street Philadelphia, PA 19104.
Prev Med Rep. 2014;1:3-8. doi: 10.1016/j.pmedr.2014.08.001.
To evaluate gastrointestinal and cardiovascular adverse event risks associated with optical colonoscopy (OC) among Medicare outpatients who received computed tomography colonography (CTC) as their initial method of colorectal evaluation.
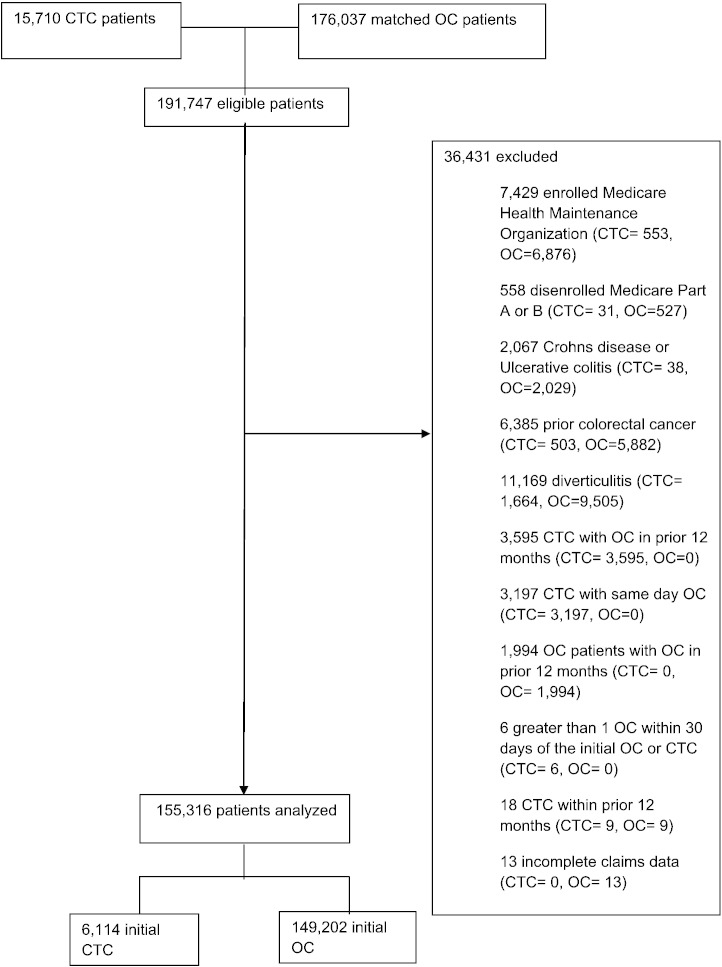
Medicare claims were compared between 6,114 outpatients ≥ 66 years who received initial CTC and 149,202 outpatients who received initial OC between January 2007 and December 2008. OC patients were matched on county of residence and year of evaluation. Outcomes included lower gastrointestinal bleeding, gastrointestinal perforation, other gastrointestinal events and cardiovascular events resulting in an emergency department visit or hospitalization within 30 days.
Among 1,000 outpatients undergoing initial CTC, 12.4 experienced lower gastrointestinal bleeding, 0.7 perforation, 18.0 other gastrointestinal events and 45.5 cardiovascular events within 30 days. After multivariate adjustment, risks of lower gastrointestinal bleeding, other gastrointestinal events and cardiovascular events were higher with initial OC than CTC, with or without subsequent OC (OR 1.91 95CI [1.47,2.49], OR 1.35 95CI [1.07,1.69] and OR 1.38 95CI [1.18,1.62], respectively); however, perforation risk did not differ (p=0.10). This pattern is similar in older and symptomatic populations.
Rates of gastrointestinal bleeding, other gastrointestinal events and cardiovascular events are lower following initial CTC than OC, but rates of perforation do not differ.
评估在接受计算机断层扫描结肠成像(CTC)作为其结直肠癌初始评估方法的医疗保险门诊患者中,光学结肠镜检查(OC)相关的胃肠道和心血管不良事件风险。
比较了2007年1月至2008年12月期间6114名年龄≥66岁接受初始CTC的门诊患者和149202名接受初始OC的门诊患者的医疗保险理赔情况。OC患者按居住县和评估年份进行匹配。结局包括下消化道出血、胃肠道穿孔、其他胃肠道事件以及导致在30天内前往急诊科就诊或住院的心血管事件。
在1000名接受初始CTC的门诊患者中,30天内有12.4例发生下消化道出血,0.7例发生穿孔,18.0例发生其他胃肠道事件,45.5例发生心血管事件。多因素调整后,无论是否进行后续OC,初始OC组的下消化道出血、其他胃肠道事件和心血管事件风险均高于CTC组(OR分别为1.91,95%CI[1.47,2.49];OR为1.35,95%CI[1.07,1.69];OR为1.38,95%CI[1.18,1.62]);然而,穿孔风险无差异(p = 0.10)。在老年人群和有症状人群中这种模式相似。
初始CTC后胃肠道出血、其他胃肠道事件和心血管事件的发生率低于OC,但穿孔发生率无差异。