Chu Xiangyang, Hou Xiaobin, Zhang Lianbin, Xue Zhiqiang, Ren Zhipeng, Wen Jiaxin, Liu Yi, Ma Kefeng, Sun Yu'e
Department of Thoracic Surgery, PLA General Hospital, Beijing 100853, China.
Zhongguo Fei Ai Za Zhi. 2014 Dec;17(12):845-9. doi: 10.3779/j.issn.1009-3419.2014.12.04.
Localization of pulmonary ground glass small nodule is the technical difficulty of minimally invasive operation resection. The aim of this study is to evaluate the value of intraoperative computed tomography (CT)-guided localization using a hook-wire system for small ground glass opacity (GGO) in minimally invasive resection, as well as to discuss the necessity and feasibility of surgical resection of small GGOs (<10 mm) through a minimally invasive approach.
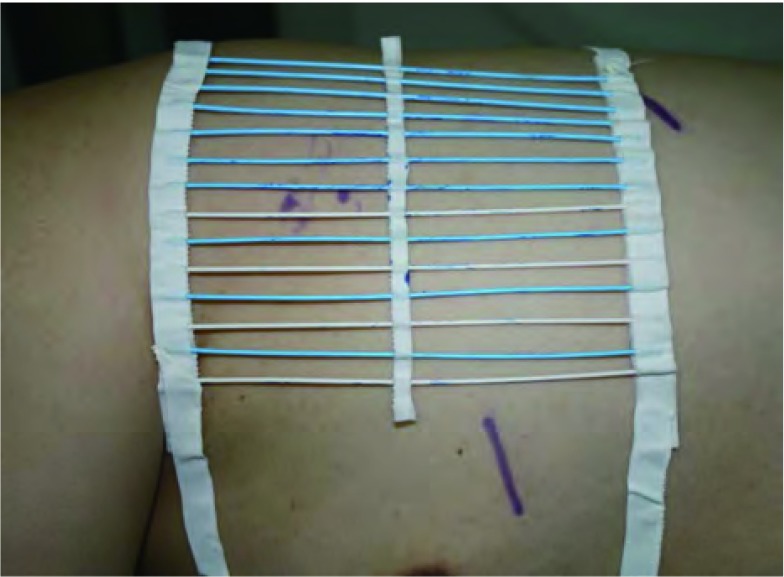
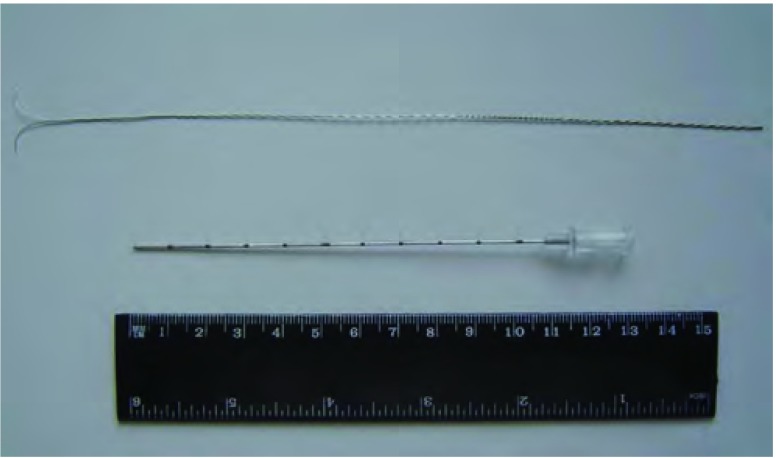
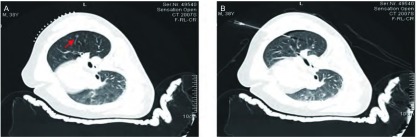
The records of 32 patients with 41 small GGOs who underwent intraoperative CT-guided double-thorn hook wire localization prior to video-assisted thoracoscopic wedge resection from October 2009 to October 2013 were retrospectively reviewed. All patients received video-assisted thoracoscopic surgery (VATS) within 10 min after wire localization. The efficacy of intraoperative localization was evaluated in terms of procedure time, VATS success rate, and associated complications of localization.
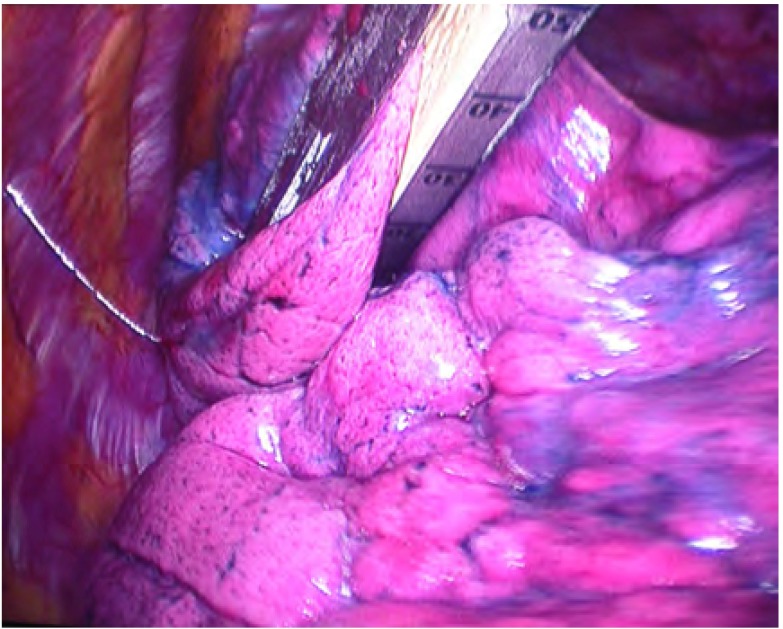
A total of 32 patients (15 males and 17 females) underwent 41 VATS resections, with 2 simultaneous nodule resections performed in 3 patients, 3 lesion resections in 1 patient, and 5 lesions in a patient. Nodule diameters ranged from 2 mm-10 mm (mean: 5 mm). The distance of lung lesions from the nearest pleural surfaces ranged within 5 mm-24 mm (mean: 12.5 mm). All resections of lesions guided by the inserted hook wires were successfully performed by VATS (100% success rate). The mean procedure time for the CT-guided hook wire localization was 8.4 min (range: 4 min-18 min). The mean procedure time for VATS was 32 min (range: 14 min-98 min). The median hospital time was 8 d (range: 5 d-14 d). Results of pathological examination revealed 28 primary lung cancers, 9 atypical adenomatous hyperplasia, and 4 nonspecific chronic inflammations. No major complication related to the intraoperative hook wire localization and VATS was noted.
Intraoperative CT-guided hook wire localization is useful, particularly in small GGO localization in VATS wedge resection and has a significantly low rate of minor complications. Lung GGOs carry a 90% risk of malignancy. Aggressive surgical resection of these GGOs is necessary and feasible through the guidance of intraoperative CT localization technique.
肺磨玻璃小结节的定位是微创切除手术的技术难点。本研究旨在评估术中计算机断层扫描(CT)引导下使用钩丝系统对微小磨玻璃影(GGO)进行微创切除的价值,并探讨通过微创方法手术切除小GGO(<10 mm)的必要性和可行性。
回顾性分析2009年10月至2013年10月期间32例患有41个小GGO的患者的记录,这些患者在电视辅助胸腔镜楔形切除术前接受了术中CT引导下的双刺钩丝定位。所有患者在钢丝定位后10分钟内接受了电视辅助胸腔镜手术(VATS)。从手术时间、VATS成功率和定位相关并发症方面评估术中定位的效果。
共有32例患者(15例男性和17例女性)接受了41次VATS切除,其中3例患者同时切除2个结节,1例患者切除3个病灶,1例患者切除5个病灶。结节直径范围为2 mm至10 mm(平均:5 mm)。肺病灶距最近胸膜表面的距离在5 mm至24 mm范围内(平均:12.5 mm)。所有通过插入的钩丝引导的病灶切除均通过VATS成功完成(成功率100%)。CT引导下钩丝定位的平均手术时间为8.4分钟(范围:4分钟至18分钟)。VATS的平均手术时间为32分钟(范围:14分钟至98分钟)。中位住院时间为8天(范围:5天至14天)。病理检查结果显示28例原发性肺癌,9例非典型腺瘤样增生,4例非特异性慢性炎症。未发现与术中钩丝定位和VATS相关的重大并发症。
术中CT引导下钩丝定位是有用的,特别是在VATS楔形切除术中对小GGO的定位,且轻微并发症发生率极低。肺GGO有90%的恶性风险。通过术中CT定位技术的引导,积极手术切除这些GGO是必要且可行的。