Song Byung-Cheol, Cho Yoo-Kyung, Jwa Hyeyoung, Choi Eun Kwang, Kim Heung Up, Song Hyun Joo, Na Soo-Young, Boo Sun-Jin, Jeong Seung Uk
Department of Internal Medicine, Jeju National University School of Medicine, Jeju, Korea.
Clin Mol Hepatol. 2014 Dec;20(4):355-60. doi: 10.3350/cmh.2014.20.4.355. Epub 2014 Dec 24.
BACKGROUND/AIMS: Spontaneous HBeAg seroconversion occurs frequently in the immune reactive phase in HBeAg-positive chronic hepatitis B (CHB). Therefore, observation for 3-6 months before commencing antiviral therapy is recommended in patients with alanine aminotransferase (ALT) levels that exceed twice the upper limit of normal (ULN). However, HBeAg seroconversion occurs infrequently in patients infected with hepatitis B virus (HBV) genotype C. The aim of the present study was to determine whether the waiting policy is necessary in endemic areas of HBV genotype C infection.
Ninety patients with HBeAg-positive CHB were followed prospectively without administering antiviral therapy for 6 months. Antiviral therapy was initiated promptly at any time if there was any evidence of biochemical (i.e., acute exacerbation of HBV infection or aggravation of jaundice) or symptomatic deterioration. After 6 months of observation, antiviral therapy was initiated according to the patient's ALT and HBV DNA levels.
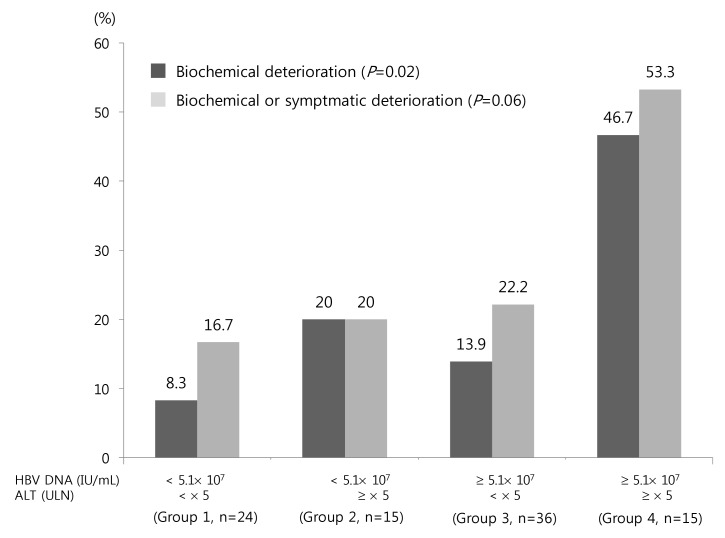
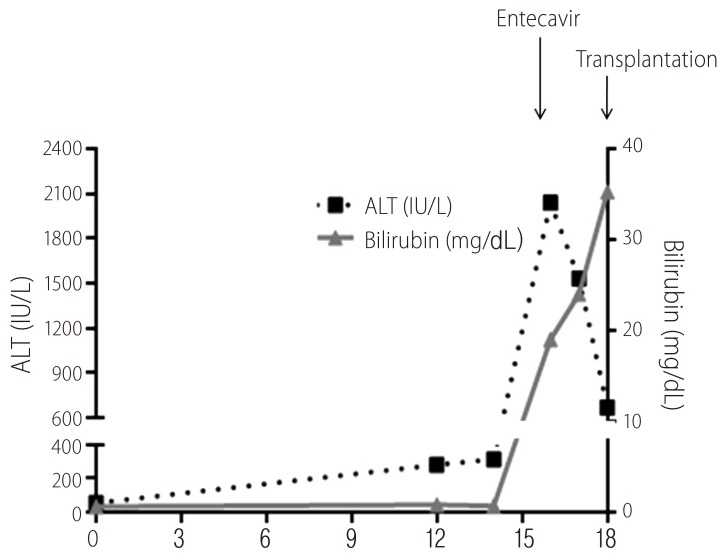
Only one patient (1.1%) achieved spontaneous HBeAg seroconversion. Biochemical and symptomatic deterioration occurred before 6 months in 17 patients (18.9%) and 5 patients, respectively. High ALT and HBV DNA levels were both independent risk factors for biochemical deterioration. Of 15 patients with HBV DNA ≥ 5.1 × 10(7) IU/mL and ALT ≥ 5 × ULN, biochemical deterioration occurred in 7 (46.7%), including 1 patient receiving liver transplantation due to liver failure.
Spontaneous HBeAg seroconversion in patients with HBeAg-positive CHB is rare within 6 months. Biochemical deterioration was common and may lead to liver failure. Immediate antiviral therapy should be considered, especially in patients with high ALT and HBV DNA levels in endemic areas of genotype C infection.
背景/目的:在HBeAg阳性慢性乙型肝炎(CHB)的免疫反应期,HBeAg常自发血清学转换。因此,对于丙氨酸氨基转移酶(ALT)水平超过正常上限(ULN)两倍的患者,建议在开始抗病毒治疗前观察3 - 6个月。然而,在感染乙型肝炎病毒(HBV)C基因型的患者中,HBeAg血清学转换很少发生。本研究的目的是确定在HBV C基因型感染流行地区,等待策略是否必要。
对90例HBeAg阳性CHB患者进行前瞻性随访,6个月内不给予抗病毒治疗。如果有任何生化指标恶化(即HBV感染急性加重或黄疸加重)或症状恶化的证据,则随时立即开始抗病毒治疗。观察6个月后,根据患者的ALT和HBV DNA水平开始抗病毒治疗。
仅1例患者(1.1%)实现了HBeAg自发血清学转换。分别有17例患者(18.9%)和5例患者在6个月前出现了生化指标恶化和症状恶化。高ALT和HBV DNA水平均是生化指标恶化的独立危险因素。在15例HBV DNA≥5.1×10⁷IU/mL且ALT≥5×ULN的患者中,7例(46.7%)出现了生化指标恶化,其中1例因肝衰竭接受了肝移植。
HBeAg阳性CHB患者在6个月内HBeAg自发血清学转换很少见。生化指标恶化很常见,可能导致肝衰竭。应考虑立即进行抗病毒治疗,尤其是在C基因型感染流行地区,ALT和HBV DNA水平高的患者。