Agweyu Ambrose, Gathara David, Oliwa Jacquie, Muinga Naomi, Edwards Tansy, Allen Elizabeth, Maleche-Obimbo Elizabeth, English Mike
Health Services Unit, Kenya Medical Research Institute (KEMRI)-Wellcome Trust Research Programme, Nairobi.
Medical Research Council Tropical Epidemiology Group, Department of Infectious Disease Epidemiology.
Clin Infect Dis. 2015 Apr 15;60(8):1216-24. doi: 10.1093/cid/ciu1166. Epub 2014 Dec 30.
There are concerns that the evidence from studies showing noninferiority of oral amoxicillin to benzyl penicillin for severe pneumonia may not be generalizable to high-mortality settings.
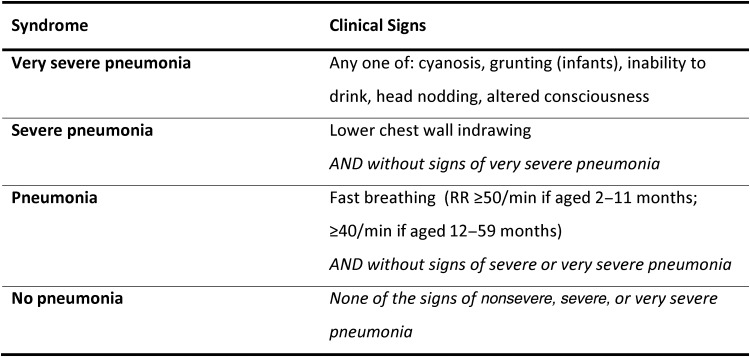
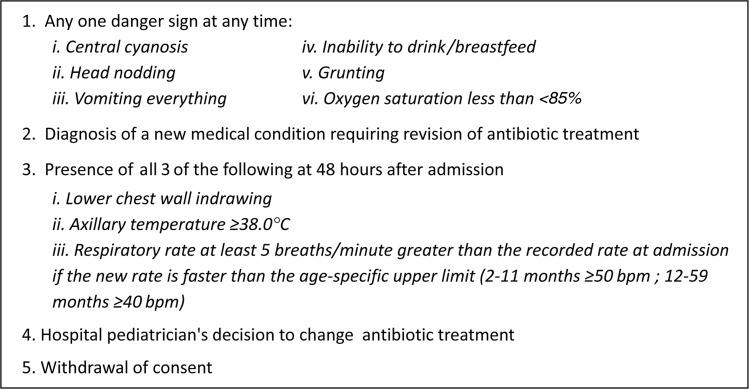
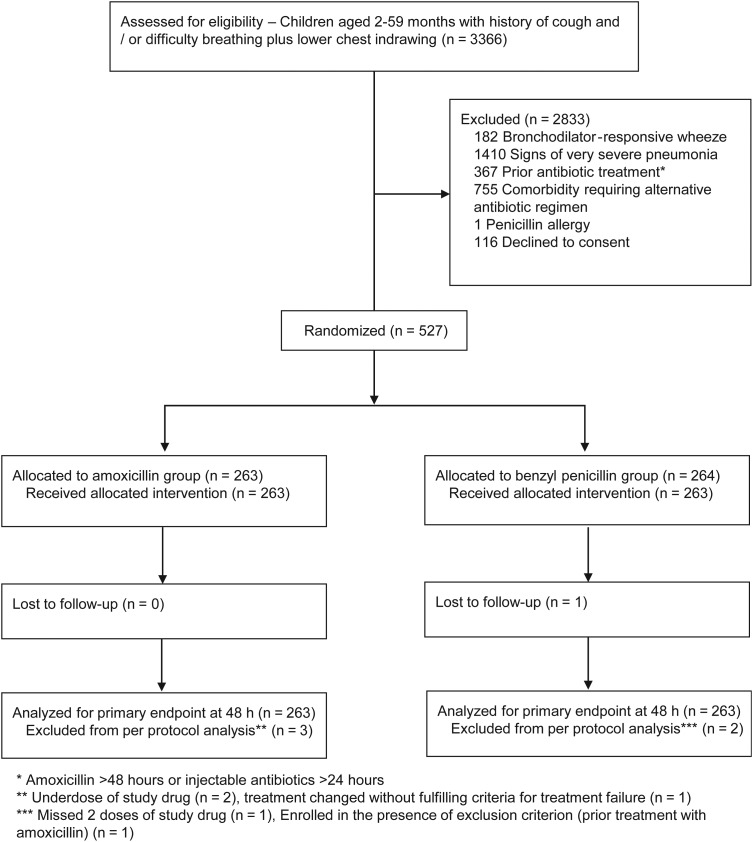
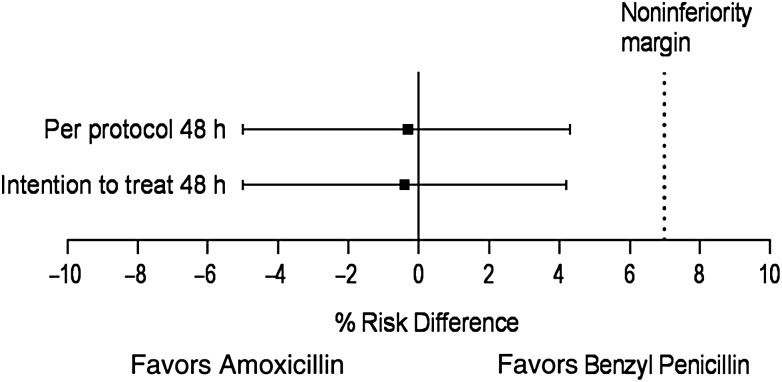
An open-label, multicenter, randomized controlled noninferiority trial was conducted at 6 Kenyan hospitals. Eligible children aged 2-59 months were randomized to receive amoxicillin or benzyl penicillin and followed up for the primary outcome of treatment failure at 48 hours. A noninferiority margin of risk difference between amoxicillin and benzyl penicillin groups was prespecified at 7%.
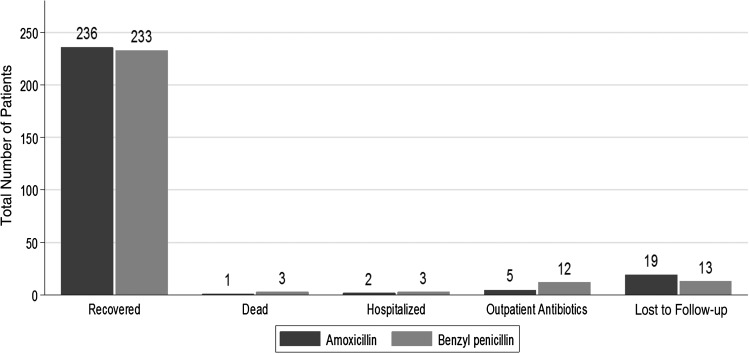
We recruited 527 children, including 302 (57.3%) with comorbidity. Treatment failure was observed in 20 of 260 (7.7%) and 21 of 261 (8.0%) of patients in the amoxicillin and benzyl penicillin arms, respectively (risk difference, -0.3% [95% confidence interval, -5.0% to 4.3%]) in per-protocol analyses. These findings were supported by the results of intention-to-treat analyses. Treatment failure by day 5 postenrollment was 11.4% and 11.0% and rising to 13.5% and 16.8% by day 14 in the amoxicillin vs benzyl penicillin groups, respectively. The most frequent cause of cumulative treatment failure at day 14 was clinical deterioration within 48 hours of enrollment (33/59 [55.9%]). Four patients died (overall mortality 0.8%) during the study, 3 of whom were allocated to the benzyl penicillin group. The presence of wheeze was independently associated with less frequent treatment failure.
Our findings confirm noninferiority of amoxicillin to benzyl penicillin, provide estimates of risk of treatment failure in Kenya, and offer important additional evidence for policy making in sub-Saharan Africa.
NCT01399723.
有担忧认为,显示口服阿莫西林治疗重症肺炎不劣于苄星青霉素的研究证据可能无法推广至高死亡率环境。
在肯尼亚的6家医院开展了一项开放标签、多中心、随机对照非劣效性试验。符合条件的2至59个月大儿童被随机分配接受阿莫西林或苄星青霉素治疗,并对48小时时治疗失败的主要结局进行随访。阿莫西林组与苄星青霉素组之间预先设定的风险差异非劣效界值为7%。
我们招募了527名儿童,其中302名(57.3%)患有合并症。在符合方案分析中,阿莫西林组和苄星青霉素组分别有260名患者中的20名(7.7%)和261名患者中的21名(8.0%)出现治疗失败(风险差异为-0.3% [95%置信区间,-5.0%至4.3%])。这些发现得到了意向性分析结果的支持。入组后第5天的治疗失败率在阿莫西林组和苄星青霉素组分别为11.4%和11.0%,到第14天分别升至13.5%和16.8%。第14天累积治疗失败的最常见原因是入组后48小时内临床病情恶化(33/59 [55.9%])。研究期间有4名患者死亡(总死亡率0.8%),其中3名被分配至苄星青霉素组。喘息的存在与治疗失败频率较低独立相关。
我们的研究结果证实了阿莫西林不劣于苄星青霉素,提供了肯尼亚治疗失败风险的估计值,并为撒哈拉以南非洲的政策制定提供了重要的补充证据。
NCT01399723。