Ongolo-Zogo Pierre, Lavis John N, Tomson Goran, Sewankambo Nelson K
Health Policy and Knowledge Translation Doctoral Program, Makerere University College of Health Sciences, P,O, Box 7072, Kampala, Uganda.
Health Res Policy Syst. 2015 Jan 1;13:2. doi: 10.1186/1478-4505-13-2.
There is a scarcity of empirical data on African country climates for evidence-informed health system policymaking (EIHSP) to backup the longstanding reputation that research evidence is not valued enough by health policymakers as an information input.Herein, we assess whether and how changes have occurred in the climate for EIHSP before and after the establishment of two Knowledge Translation Platforms housed in government institutions in Cameroon and Uganda since 2006.
We merged content analysis techniques and policy sciences analytical frameworks to guide this structured review of governmental policy documents geared at achieving health Millennium Development Goals. We combined i) a quantitative exploration of the usage statistics of research-related words and constructs, citations of types of evidence, and budgets allocated to research-related activities; and (ii) an interpretive exploration using a deductive thematic analysis approach to uncover changes in the institutions, interests, ideas, and external factors displaying the country climate for EIHSP. Descriptive statistics compared quantitative data across countries during the periods 2001-2006 and 2007-2012.
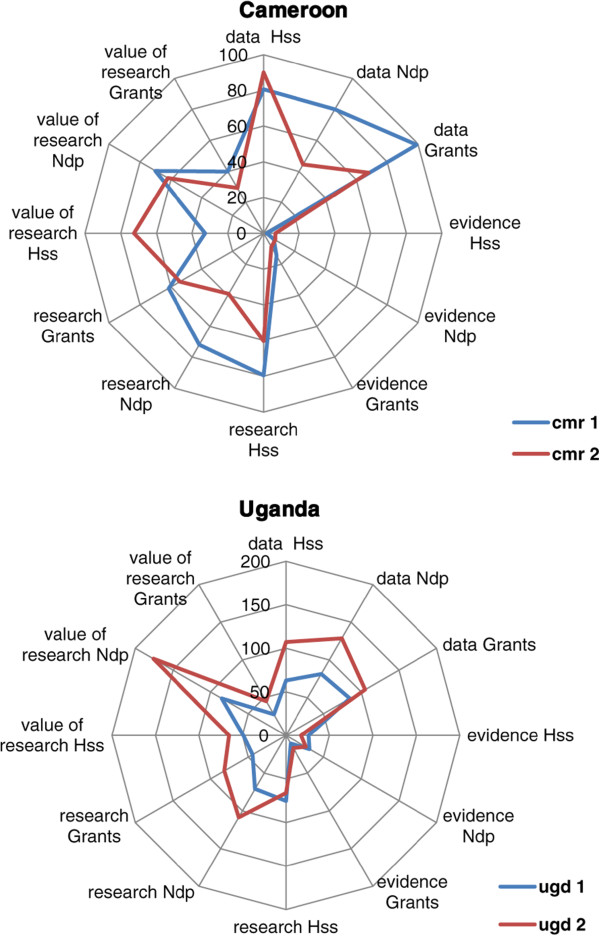
We reviewed 54 documents, including 33 grants approved by global health initiatives. The usage statistics of research-related words and constructs showed an increase over time across countries. Varied forms of data, information, or research were instrumentally used to describe the burden and determinants of poverty and health conditions. The use of evidence syntheses to frame poverty and health problems, select strategies, or forecast the expected outcomes has remained sparse over time and across countries. The budgets for research increased over time from 28.496 to 95.467 million Euros (335%) in Cameroon and 38.064 to 58.884 million US dollars (155%) in Uganda, with most resources allocated to health sector performance monitoring and evaluation. The consistent naming of elements pertaining to the climate for EIHSP features the greater influence of external donors through policy transfer.
This structured review of governmental policy documents illustrates the nascent conducive climate for EIHSP in Cameroon and Uganda and the persistent undervalue of evidence syntheses. Global and national health stakeholders should raise the profile of evidence syntheses (e.g., systematic reviews) as an information input when shaping policies and programmes.
非洲国家气候方面的实证数据匮乏,难以支持基于证据的卫生系统决策(EIHSP),以反驳长期以来关于卫生政策制定者对研究证据作为信息输入重视不足的说法。在此,我们评估自2006年以来喀麦隆和乌干达政府机构设立两个知识转化平台前后,EIHSP的气候是否以及如何发生了变化。
我们融合了内容分析技术和政策科学分析框架,以指导对旨在实现卫生千年发展目标的政府政策文件进行结构化审查。我们结合了:(i)对与研究相关的词汇和结构的使用统计、证据类型的引用以及分配给研究相关活动的预算进行定量探索;(ii)使用演绎主题分析方法进行解释性探索,以揭示体现EIHSP国家气候的机构、利益、观念和外部因素的变化。描述性统计比较了2001 - 2006年和2007 - 2012年期间各国的定量数据。
我们审查了54份文件,包括全球卫生倡议批准的33项拨款。与研究相关的词汇和结构的使用统计显示,各国随时间有所增加。各种形式的数据、信息或研究被用于描述贫困和健康状况的负担及决定因素。随着时间推移和各国情况,使用证据综合来构建贫困和健康问题、选择策略或预测预期结果的情况仍然很少。喀麦隆的研究预算从2849.6万欧元增加到9546.7万欧元(增长335%),乌干达从3806.4万美元增加到5888.4万美元(增长155%),大部分资源用于卫生部门绩效监测和评估。与EIHSP气候相关要素的持续命名体现了外部捐助者通过政策转移产生的更大影响。
对政府政策文件的这种结构化审查表明,喀麦隆和乌干达出现了有利于EIHSP的初步气候,且证据综合一直未得到充分重视。全球和国家卫生利益相关者在制定政策和计划时,应提高证据综合(如系统评价)作为信息输入的地位。