Demeester Simke, Keymeulen Bart, Kaufman Leonard, Van Dalem Annelien, Balti Eric V, Van de Velde Ursule, Goubert Patrick, Verhaeghen Katrijn, Davidson Howard W, Wenzlau Janet M, Weets Ilse, Pipeleers Daniel G, Gorus Frans K
Diabetes Research Center and University Hospital Brussels (UZ Brussel), Vrije Universiteit Brussel, Brussels, Belgium.
Barbara Davis Center for Childhood Diabetes, University of Colorado at Denver, Aurora, CO.
Diabetes Care. 2015 Apr;38(4):644-51. doi: 10.2337/dc14-1575. Epub 2015 Jan 12.
Immune intervention trials in recent-onset type 1 diabetes would benefit from biomarkers associated with good therapeutic response. In the previously reported randomized placebo-controlled anti-CD3 study (otelixizumab; GlaxoSmithKline), we tested the hypothesis that specific diabetes autoantibodies might serve this purpose.
In the included patients (n = 40 otelixizumab, n = 40 placebo), β-cell function was assessed as area under the curve (AUC) C-peptide release during a hyperglycemic glucose clamp at baseline (median duration of insulin treatment: 6 days) and every 6 months until 18 months after randomization. (Auto)antibodies against insulin (I[A]A), GAD (GADA), IA-2 (IA-2A), and ZnT8 (ZnT8A) were determined on stored sera by liquid-phase radiobinding assay.
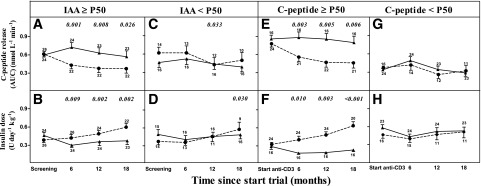
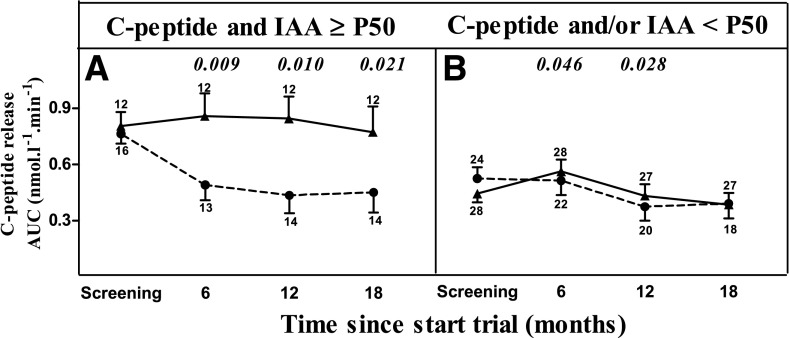
At baseline, only better preserved AUC C-peptide release and higher levels of IAA were associated with better preservation of β-cell function and lower insulin needs under anti-CD3 treatment. In multivariate analysis, IAA (P = 0.022) or the interaction of IAA and C-peptide (P = 0.013) independently predicted outcome together with treatment. During follow-up, good responders to anti-CD3 treatment (i.e., IAA(+) participants with relatively preserved β-cell function [≥ 25% of healthy control subjects]) experienced a less pronounced insulin-induced rise in I(A)A and lower insulin needs. GADA, IA-2A, and ZnT8A levels were not influenced by anti-CD3 treatment, and their changes showed no relation to functional outcome.
There is important specificity of IAA among other diabetes autoantibodies to predict good therapeutic response of recent-onset type 1 diabetic patients to anti-CD3 treatment. If confirmed, future immune intervention trials in type 1 diabetes should consider both relatively preserved functional β-cell mass and presence of IAA as inclusion criteria.
近期发病的1型糖尿病免疫干预试验将受益于与良好治疗反应相关的生物标志物。在先前报道的随机安慰剂对照抗CD3研究(otexizumab;葛兰素史克公司)中,我们检验了特定糖尿病自身抗体可能符合这一目的的假设。
纳入的患者(n = 40例otexizumab组,n = 40例安慰剂组),在基线时(胰岛素治疗中位持续时间:6天)以及随机分组后每6个月直至18个月,通过高血糖葡萄糖钳夹试验评估β细胞功能,以曲线下面积(AUC)表示C肽释放量。采用液相放射结合试验测定储存血清中抗胰岛素(I[A]A)、谷氨酸脱羧酶(GADA)、胰岛抗原2(IA - 2A)和锌转运体8(ZnT8A)的(自身)抗体。
在基线时,仅更好保留的AUC C肽释放量和更高水平的IAA与抗CD3治疗下更好地保留β细胞功能及更低的胰岛素需求相关。在多变量分析中,IAA(P = 0.022)或IAA与C肽的相互作用(P = 0.013)与治疗一起独立预测结局。在随访期间,抗CD3治疗的良好反应者(即具有相对保留的β细胞功能[≥健康对照受试者的25%]的IAA(+)参与者)胰岛素诱导的I(A)A升高不明显且胰岛素需求较低。GADA、IA - 2A和ZnT8A水平不受抗CD3治疗影响,其变化与功能结局无关。
在其他糖尿病自身抗体中,IAA对于预测近期发病的1型糖尿病患者对抗CD3治疗的良好治疗反应具有重要特异性。如果得到证实,未来1型糖尿病免疫干预试验应考虑将相对保留的功能性β细胞量和IAA的存在作为纳入标准。