School of Health Administration, College of Allied Health Professions, Texas State University, San Marcos, TX, United States.
JMIR Med Inform. 2014 Sep 30;2(2):e26. doi: 10.2196/medinform.3625.
Although health information exchanges (HIE) have existed since their introduction by President Bush in his 2004 State of the Union Address, and despite monetary incentives earmarked in 2009 by the health information technology for economic and clinical health (HITECH) Act, adoption of HIE has been sparse in the United States. Research has been conducted to explore the concept of HIE and its benefit to patients, but viable business plans for their existence are rare, and so far, no research has been conducted on the dynamic nature of barriers over time.
The aim of this study is to map the barriers mentioned in the literature to illustrate the effect, if any, of barriers discussed with respect to the HITECH Act from 2009 to the early months of 2014.
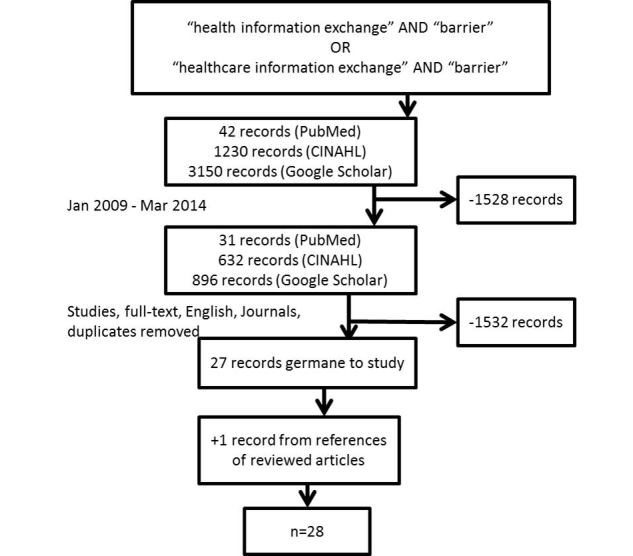
We conducted a systematic literature review from CINAHL, PubMed, and Google Scholar. The search criteria primarily focused on studies. Each article was read by at least two of the authors, and a final set was established for evaluation (n=28).
The 28 articles identified 16 barriers. Cost and efficiency/workflow were identified 15% and 13% of all instances of barriers mentioned in literature, respectively. The years 2010 and 2011 were the most plentiful years when barriers were discussed, with 75% and 69% of all barriers listed, respectively.
The frequency of barriers mentioned in literature demonstrates the mindfulness of users, developers, and both local and national government. The broad conclusion is that public policy masks the effects of some barriers, while revealing others. However, a deleterious effect can be inferred when the public funds are exhausted. Public policy will need to lever incentives to overcome many of the barriers such as cost and impediments to competition. Process improvement managers need to optimize the efficiency of current practices at the point of care. Developers will need to work with users to ensure tools that use HIE resources work into existing workflows.
尽管自布什总统在 2004 年国情咨文中提出健康信息交换(HIE)以来,HIE 就已经存在,并且尽管 2009 年的《健康信息技术经济和临床健康法案》(HITECH 法案)专门为此提供了资金激励,但 HIE 的采用在美国仍然很少。人们已经对 HIE 的概念及其对患者的益处进行了研究,但很少有可行的商业计划来支持其存在,而且到目前为止,还没有针对随着时间的推移障碍的动态性质进行研究。
本研究旨在对文献中提到的障碍进行映射,以说明 2009 年至 2014 年初 HITECH 法案期间讨论的障碍对 HIE 的影响(如果有影响的话)。
我们从 CINAHL、PubMed 和 Google Scholar 进行了系统的文献回顾。搜索标准主要侧重于研究。每篇文章至少由两位作者阅读,并最终确定了一组进行评估(n=28)。
确定的 28 篇文章共确定了 16 个障碍。成本和效率/工作流程分别占文献中提到的障碍的 15%和 13%。讨论障碍最多的年份是 2010 年和 2011 年,分别占列出的所有障碍的 75%和 69%。
文献中提到的障碍的频率表明了用户、开发者以及地方和国家政府的关注。广泛的结论是,公共政策掩盖了一些障碍的影响,同时又揭示了另一些障碍的影响。但是,当公共资金耗尽时,可以推断出不利影响。公共政策将需要利用激励措施来克服许多障碍,例如成本和竞争障碍。流程改进经理需要在护理点优化当前实践的效率。开发人员将需要与用户合作,确保使用 HIE 资源的工具能够融入现有的工作流程。