Moshabela Mosa, Sene Massamba, Nanne Ingrid, Tankoano Yombo, Schaefer Jennifer, Niang Oumulkhairy, Sachs Sonia Ehrlich
Department of Rural Health, School of Nursing and Public Health, University of KwaZulu-Natal, Science Drive, Howard College, Fourth Floor, George Campbell Building, Durban, 4001, South Africa.
Millennium Promise, Columbia University, Dakar, Senegal.
BMC Health Serv Res. 2015 Jan 22;15:16. doi: 10.1186/s12913-014-0664-4.
Reliable detection of maternal deaths is an essential prerequisite for successful diagnosis of barriers to care and formulation of relevant targeted interventions. In a community-level case study, the use of household-level surveillance in Senegal unveiled an apparent increase in maternal deaths, which triggered a rapid-cycle collaborative response to implement a multipronged set of quick-win and sustained interventions intended to improve quality care.
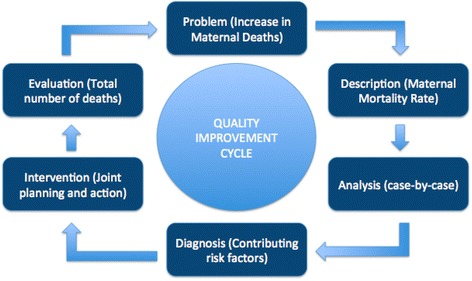
Part of a multi-country effort, the Millennium Villages Project is implementing a routine community-level information system in Senegal, able to detect maternal deaths in real-time and uncover clinical and social factors contributing to mortality. Within this geographically demarcated area of approximately 32 000 inhabitants, with a well-structured health system with patient referral services, deaths were registered and notified by community health workers, followed by timely verbal and social autopsies. Using the Pathway to Survival conceptual framework, case analysis and mortality reviews were conducted for evaluation and quality improvement purposes.
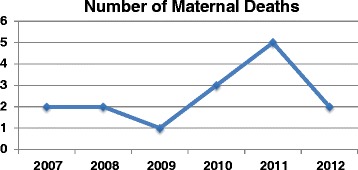
The estimated maternal mortality rates rose from 67/100000 births in 2009 (1 death), to 202/100000 births in 2010 (3 deaths) and 392/100000 births (5 deaths) in 2011. Although absolute numbers of maternal deaths remained too small for robust statistical analysis, following verbal autopsy analyses in 2011, it became evident that an unexpectedly high proportion of maternal deaths were occurring at the referral hospital, mostly post-Caesarian section. Inadequate case management of post-partum haemorrhage at the referral hospital was the most frequently identified probable cause of death. A joint task team systematically identified several layers of inefficiencies, with a potential negative impact on a larger catchment area than the study community.
In this study, routine community-based surveillance identified inefficiencies at a tertiary level of care. Community-level surveillance systems that include pregnancy, birth and death tracking through household visits by community health workers , combined with verbal and social autopsy can identify barriers within the continuum of maternal care. Use of mHealth data collection tools sensitive enough to detect small changes in community-level mortality trends in real-time, can facilitate rapid-cycle quality improvement interventions, particularly when associated with social accountability structures of mortality reviews.
可靠地检测孕产妇死亡情况是成功诊断护理障碍并制定相关针对性干预措施的重要前提。在一项社区层面的案例研究中,塞内加尔采用家庭层面监测揭示了孕产妇死亡人数明显增加,这引发了快速循环的协作应对措施,以实施一系列旨在改善优质护理的多管齐下的速赢和持续干预措施。
作为多国努力的一部分,千年村项目正在塞内加尔实施一个常规社区层面信息系统,该系统能够实时检测孕产妇死亡情况,并揭示导致死亡的临床和社会因素。在这个约有32000名居民、拥有结构完善的卫生系统及患者转诊服务的地理划定区域内,社区卫生工作者对死亡情况进行登记和通报,随后及时进行口头和社会尸检。利用“生存途径”概念框架,为评估和质量改进目的进行了案例分析和死亡率审查。
估计的孕产妇死亡率从2009年的每10万例分娩67例(1例死亡),上升至2010年的每10万例分娩202例(3例死亡)以及2011年的每10万例分娩392例(5例死亡)。尽管孕产妇死亡的绝对数量仍然太少,无法进行有力的统计分析,但在2011年进行口头尸检分析后,很明显有出乎意料高比例的孕产妇死亡发生在转诊医院,大多是剖宫产术后。转诊医院对产后出血的病例管理不足是最常确定的可能死因。一个联合任务小组系统地识别出了几层效率低下的情况,其对更大集水区的潜在负面影响超出了研究社区范围。
在本研究中,常规的基于社区的监测发现了三级护理层面的效率低下情况。通过社区卫生工作者进行家访来跟踪妊娠、分娩和死亡情况的社区层面监测系统,再结合口头和社会尸检,能够识别孕产妇护理连续过程中的障碍。使用足够敏感以实时检测社区层面死亡率趋势微小变化的移动健康数据收集工具,可促进快速循环的质量改进干预措施,特别是当与死亡率审查的社会问责结构相关联时。