Hames Samuel C, Sinnya Sudipta, Tan Jean-Marie, Morze Conrad, Sahebian Azadeh, Soyer H Peter, Prow Tarl W
Dermatology Research Center, School of Medicine, University of Queensland, Translational Research Institute, Princess Alexandra Hospital, Brisbane, Australia.
PLoS One. 2015 Jan 23;10(1):e0112447. doi: 10.1371/journal.pone.0112447. eCollection 2015.
Clinical diagnosis of actinic keratosis is known to have intra- and inter-observer variability, and there is currently no non-invasive and objective measure to diagnose these lesions.
The aim of this pilot study was to determine if automatically detecting and circumscribing actinic keratoses in clinical photographs is feasible.
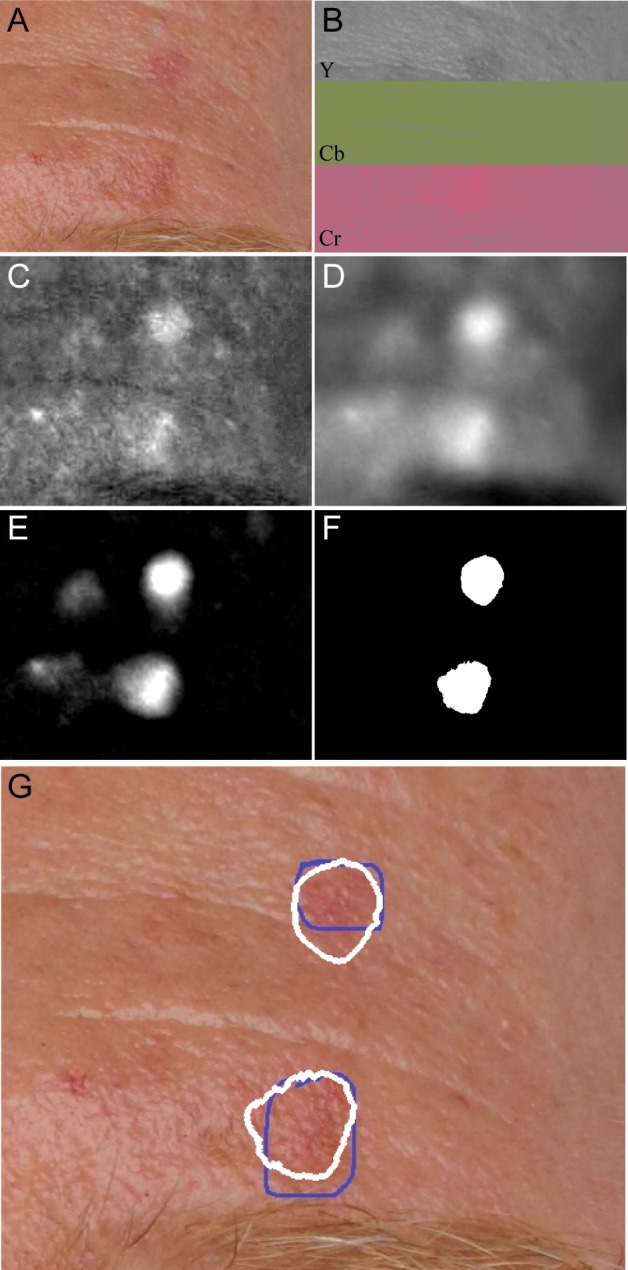
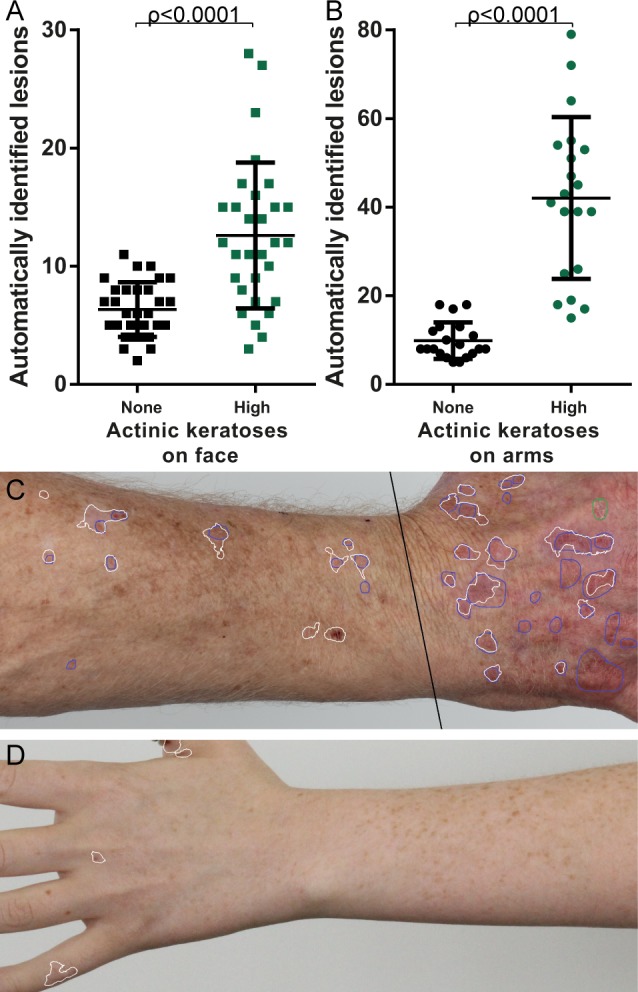
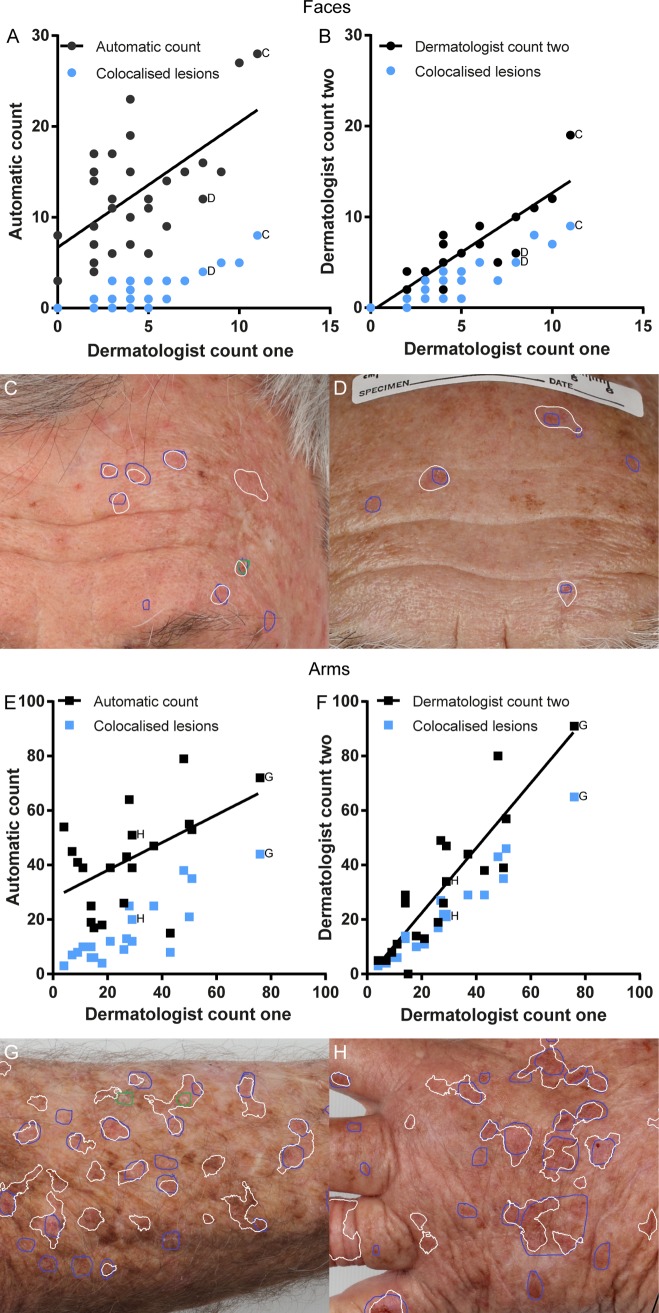
Photographs of the face and dorsal forearms were acquired in 20 volunteers from two groups: the first with at least on actinic keratosis present on the face and each arm, the second with no actinic keratoses. The photographs were automatically analysed using colour space transforms and morphological features to detect erythema. The automated output was compared with a senior consultant dermatologist's assessment of the photographs, including the intra-observer variability. Performance was assessed by the correlation between total lesions detected by automated method and dermatologist, and whether the individual lesions detected were in the same location as the dermatologist identified lesions. Additionally, the ability to limit false positives was assessed by automatic assessment of the photographs from the no actinic keratosis group in comparison to the high actinic keratosis group.
The correlation between the automatic and dermatologist counts was 0.62 on the face and 0.51 on the arms, compared to the dermatologist's intra-observer variation of 0.83 and 0.93 for the same. Sensitivity of automatic detection was 39.5% on the face, 53.1% on the arms. Positive predictive values were 13.9% on the face and 39.8% on the arms. Significantly more lesions (p<0.0001) were detected in the high actinic keratosis group compared to the no actinic keratosis group.
The proposed method was inferior to assessment by the dermatologist in terms of sensitivity and positive predictive value. However, this pilot study used only a single simple feature and was still able to achieve sensitivity of detection of 53.1% on the arms.This suggests that image analysis is a feasible avenue of investigation for overcoming variability in clinical assessment. Future studies should focus on more sophisticated features to improve sensitivity for actinic keratoses without erythema and limit false positives associated with the anatomical structures on the face.
光化性角化病的临床诊断存在观察者内和观察者间的差异,目前尚无用于诊断这些病变的非侵入性客观方法。
本初步研究的目的是确定在临床照片中自动检测和圈定光化性角化病是否可行。
从两组20名志愿者处获取面部和前臂背部的照片:第一组面部和每只手臂上至少有一处光化性角化病,第二组没有光化性角化病。使用颜色空间变换和形态学特征对照片进行自动分析以检测红斑。将自动输出结果与皮肤科高级顾问对照片的评估进行比较,包括观察者内差异。通过自动方法检测到的总病变与皮肤科医生检测到的总病变之间的相关性以及检测到的单个病变是否与皮肤科医生确定的病变位于同一位置来评估性能。此外,通过与高光化性角化病组相比自动评估无光化性角化病组的照片来评估限制假阳性的能力。
面部自动计数与皮肤科医生计数之间的相关性为0.62,手臂为0.51,而皮肤科医生的观察者内差异分别为0.83和0.93。面部自动检测的敏感性为39.5%,手臂为53.1%。面部的阳性预测值为13.9%,手臂为39.8%。高光化性角化病组检测到的病变明显多于无光化性角化病组(p<0.0001)。
就敏感性和阳性预测值而言,所提出的方法不如皮肤科医生的评估。然而,这项初步研究仅使用了一个简单特征,仍能在手臂上实现53.1%的检测敏感性。这表明图像分析是克服临床评估差异的可行研究途径。未来的研究应侧重于更复杂的特征,以提高对无红斑光化性角化病的敏感性,并限制与面部解剖结构相关的假阳性。