Koleala Tamarah, Karl Stephan, Laman Moses, Moore Brioni R, Benjamin John, Barnadas Celine, Robinson Leanne J, Kattenberg Johanna H, Javati Sarah, Wong Rina P M, Rosanas-Urgell Anna, Betuela Inoni, Siba Peter M, Mueller Ivo, Davis Timothy M E
Papua New Guinea Institute of Medical Research, Madang, Papua New Guinea.
School of Medicine and Pharmacology, University of Western Australia, Fremantle Hospital, PO Box 480, Fremantle, 6959, WA, Australia.
Malar J. 2015 Jan 28;14:37. doi: 10.1186/s12936-015-0560-3.
In northern Papua New Guinea (PNG), most Plasmodium falciparum isolates proved resistant to chloroquine (CQ) in vitro between 2005 and 2007, and there was near-fixation of pfcrt K76T, pfdhfr C59R/S108N and pfmdr1 N86Y. To determine whether the subsequent introduction of artemisinin combination therapy (ACT) and reduced CQ-sulphadoxine-pyrimethamine pressure had attenuated parasite drug susceptibility and resistance-associated mutations, these parameters were re-assessed between 2011 and 2013.
A validated fluorescence-based assay was used to assess growth inhibition of 52 P. falciparum isolates from children in a clinical trial in Madang Province. Responses to CQ, lumefantrine, piperaquine, naphthoquine, pyronaridine, artesunate, dihydroartemisinin, artemether were assessed. Molecular resistance markers were detected using a multiplex PCR ligase detection reaction fluorescent microsphere assay.
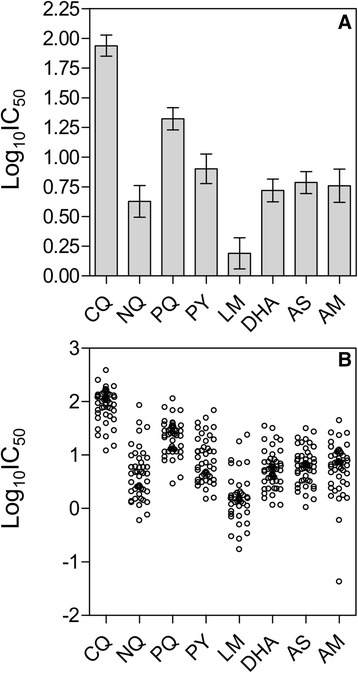
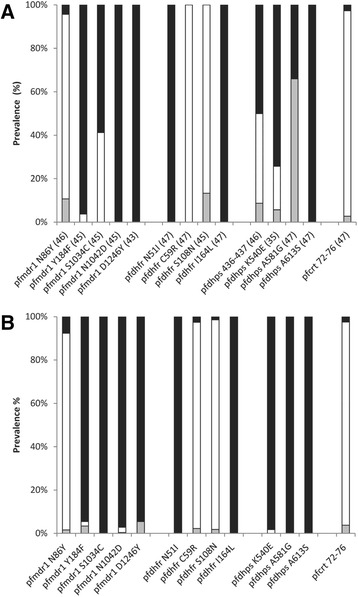
CQ resistance (in vitro concentration required for 50% parasite growth inhibition (IC₅₀) >100 nM) was present in 19% of isolates. All piperaquine and naphthoquine IC₅₀s were <100 nM and those for lumefantrine, pyronaridine and the artemisinin derivatives were in low nM ranges. Factor analysis of IC₅₀s showed three groupings (lumefantrine; CQ, piperaquine, naphthoquine; pyronaridine, dihydroartemisinin, artemether, artesunate). Most isolates (96%) were monoclonal pfcrt K76T (SVMNT) mutants and most (86%) contained pfmdr1 N86Y (YYSND). No wild-type pfdhfr was found but most isolates contained wild-type (SAKAA) pfdhps. Compared with 2005-2007, the geometric mean (95% CI) CQ IC₅₀ was lower (87 (71-107) vs 167 (141-197) nM) and there had been no change in the prevalence of pfcrt K76T or pfmdr1 mutations. There were fewer isolates of the pfdhps (SAKAA) wild-type (60 vs 100%) and pfdhfr mutations persisted.
Reflecting less drug pressure, in vitro CQ sensitivity appears to be improving in Madang Province despite continued near-fixation of pfcrt K76T and pfmdr1 mutations. Temporal changes in IC₅₀s for other anti-malarial drugs were inconsistent but susceptibility was preserved. Retention or increases in pfdhfr and pfdhps mutations reflect continued use of sulphadoxine-pyrimethamine in the study area including through paediatric intermittent preventive treatment. The susceptibility of local isolates to lumefantrine may be unrelated to those of other ACT partner drugs.
Australian New Zealand Clinical Trials Registry ACTRN12610000913077 .
在巴布亚新几内亚(PNG)北部,2005年至2007年间,多数恶性疟原虫分离株在体外被证明对氯喹(CQ)耐药,并且pfcrt K76T、pfdhfr C59R/S108N和pfmdr1 N86Y近乎固定。为了确定随后引入的青蒿素联合疗法(ACT)以及降低的CQ-磺胺多辛-乙胺嘧啶压力是否减弱了寄生虫对药物的敏感性和与耐药相关的突变,于2011年至2013年间对这些参数进行了重新评估。
在马当省的一项临床试验中,采用经过验证的基于荧光的检测方法评估了52株来自儿童的恶性疟原虫分离株的生长抑制情况。评估了对CQ、卤泛群、哌喹、萘喹、咯萘啶、青蒿琥酯、双氢青蒿素、蒿甲醚的反应。使用多重PCR连接酶检测反应荧光微球检测法检测分子耐药标志物。
19%的分离株存在CQ耐药(50%寄生虫生长抑制所需的体外浓度(IC₅₀)>100 nM)。所有哌喹和萘喹的IC₅₀均<100 nM,卤泛群、咯萘啶和青蒿素衍生物的IC₅₀处于低nM范围。IC₅₀的因子分析显示有三个分组(卤泛群;CQ、哌喹、萘喹;咯萘啶、双氢青蒿素、蒿甲醚、青蒿琥酯)。多数分离株(96%)是单克隆pfcrt K76T(SVMNT)突变体,多数(86%)含有pfmdr1 N86Y(YYSND)。未发现野生型pfdhfr,但多数分离株含有野生型(SAKAA)pfdhps。与2005 - 2007年相比,CQ的几何平均(95%CI)IC₅₀较低(87(71 - 107)对167(141 - 197)nM),并且pfcrt K76T或pfmdr1突变的流行率没有变化。pfdhps(SAKAA)野生型的分离株较少(60%对100%),并且pfdhfr突变持续存在。
反映出药物压力较小,尽管pfcrt K76T和pfmdr1突变仍近乎固定,但马当省的体外CQ敏感性似乎正在改善。其他抗疟药物IC₅₀的时间变化不一致,但敏感性得以保留。pfdhfr和pfdhps突变的保留或增加反映了磺胺多辛-乙胺嘧啶在研究地区的持续使用,包括通过儿童间歇性预防治疗。当地分离株对卤泛群的敏感性可能与其他ACT联合用药伙伴药物的敏感性无关。
澳大利亚新西兰临床试验注册中心ACTRN12610000913077 。