Keller Simon S, Richardson Mark P, Schoene-Bake Jan-Christoph, O'Muircheartaigh Jonathan, Elkommos Samia, Kreilkamp Barbara, Goh Yee Yen, Marson Anthony G, Elger Christian, Weber Bernd
Department of Molecular and Clinical Pharmacology, Institute of Translational Medicine, University of Liverpool, Liverpool, United Kingdom; Department of Radiology, Walton Centre National Health Service Foundation Trust, Liverpool, United Kingdom; Department of Clinical Neuroscience, Institute of Psychiatry, King's College London, London, United Kingdom.
Ann Neurol. 2015 May;77(5):760-74. doi: 10.1002/ana.24376. Epub 2015 Mar 13.
There are competing explanations for persistent postoperative seizures after temporal lobe surgery. One is that 1 or more particular subtypes of mesial temporal lobe epilepsy (mTLE) exist that are particularly resistant to surgery. We sought to identify a common brain structural and connectivity alteration in patients with persistent postoperative seizures using preoperative quantitative magnetic resonance imaging and diffusion tensor imaging (DTI).
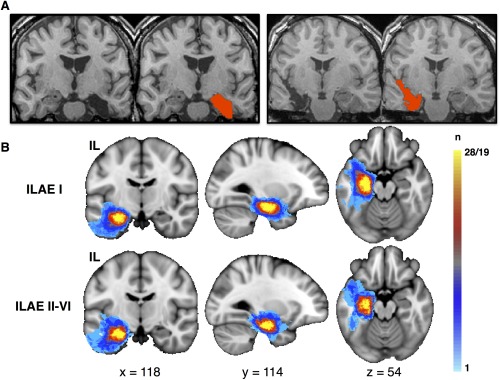
We performed a series of studies in 87 patients with mTLE (47 subsequently rendered seizure free, 40 who continued to experience postoperative seizures) and 80 healthy controls. We investigated the relationship between imaging variables and postoperative seizure outcome. All patients had unilateral temporal lobe seizure onset, had ipsilateral hippocampal sclerosis as the only brain lesion, and underwent amygdalohippocampectomy.
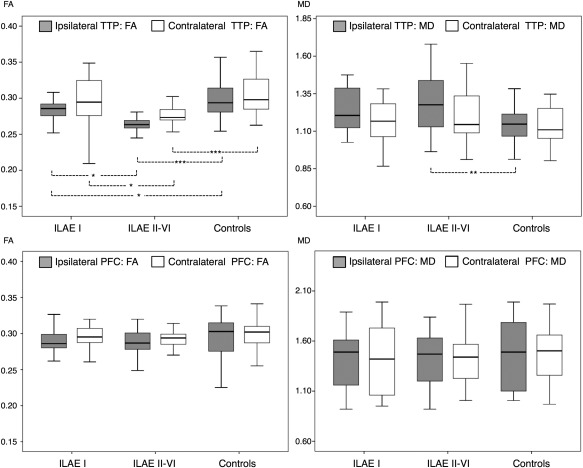
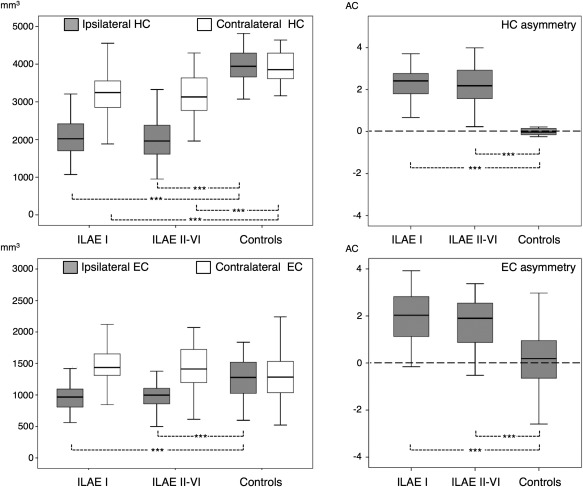
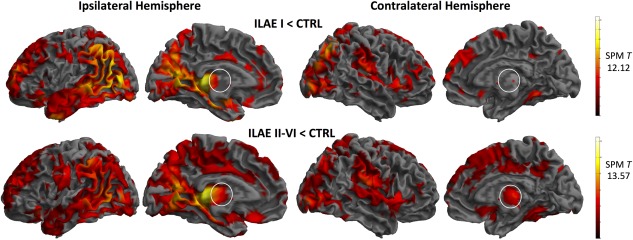
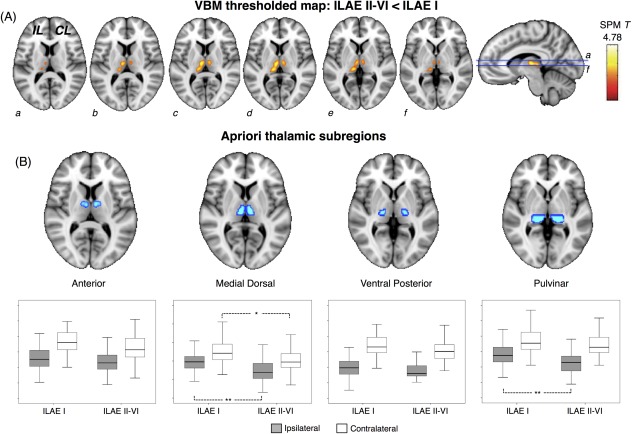
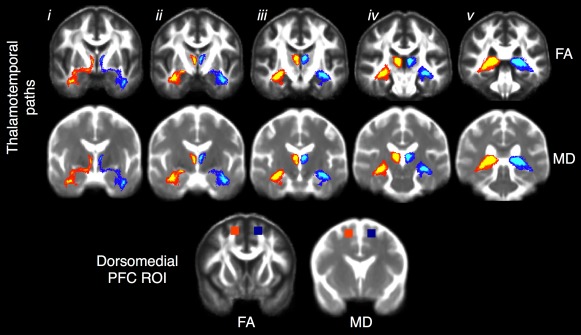
Quantitative imaging factors found not to be significantly associated with persistent seizures were volumes of ipsilateral and contralateral mesial temporal lobe structures, generalized brain atrophy, and extent of resection. There were nonsignificant trends for larger amygdala and entorhinal resections to be associated with improved outcome. However, patients with persistent seizures had significant atrophy of bilateral dorsomedial and pulvinar thalamic regions, and significant alterations of DTI-derived thalamotemporal probabilistic paths bilaterally relative to those patients rendered seizure free and controls, even when corrected for extent of mesial temporal lobe resection.
Patients with bihemispheric alterations of thalamotemporal structural networks may represent a subtype of mTLE that is resistant to temporal lobe surgery. Increasingly sensitive multimodal imaging techniques should endeavor to transform these group-based findings to individualize prediction of patient outcomes.
对于颞叶手术后持续性癫痫发作存在多种相互竞争的解释。一种观点认为,存在一种或多种特别耐药的内侧颞叶癫痫(mTLE)特定亚型。我们试图通过术前定量磁共振成像和扩散张量成像(DTI)来识别持续性术后癫痫发作患者常见的脑结构和连接改变。
我们对87例mTLE患者(47例随后癫痫发作停止,40例继续有术后癫痫发作)和80名健康对照者进行了一系列研究。我们研究了成像变量与术后癫痫发作结果之间的关系。所有患者均为单侧颞叶癫痫发作,同侧海马硬化是唯一的脑病变,并接受了杏仁核海马切除术。
定量成像因素中,同侧和对侧内侧颞叶结构体积、全脑萎缩及切除范围与持续性癫痫发作无显著相关性。杏仁核和内嗅区切除范围较大与预后改善有不显著的趋势。然而,即使校正内侧颞叶切除范围后,持续性癫痫发作患者双侧背内侧和丘脑枕叶区域仍有显著萎缩,且与癫痫发作停止的患者及对照相比,双侧DTI衍生的丘脑颞叶概率路径有显著改变。
丘脑颞叶结构网络存在双侧改变的患者可能代表了一种对颞叶手术耐药的mTLE亚型。日益敏感的多模态成像技术应致力于将这些基于群体的发现转化为对患者预后的个体化预测。