Marzano Angelo Valerio, Trevisan Valentina, Cairoli Elisa, Eller-Vainicher Cristina, Morelli Valentina, Spada Anna, Crosti Carlo, Chiodini Iacopo
Dipartimento di Fisiopatologia Medico-Chirurgica e dei Trapianti, University of Milan, Unit of Dermatology, Fondazione IRCCS Ca' Granda-Ospedale Maggiore Policlinico, Milan, Italy.
Department of Clinical Sciences and Community Health, University of Milan, Milan, Italy.
Orphanet J Rare Dis. 2015 Feb 3;10:8. doi: 10.1186/s13023-015-0230-0.
The presence of hypovitaminosis D in patients with autoimmune bullous skin diseases, such as pemphigus vulgaris (PV) and bullous pemphigoid (BP), is debated. In a previous study we found an increased prevalence of vertebral fractures (VFx) and hypovitaminosis D in PV and BP patients. The present study extends the sample size of the previous one, for investigating the 25-hydroxyvitamin D (25OHVitD) levels in relation with the skeletal health and disease intensity in these patients.
The previous study was performed in 13 PV and 15 BP patients and 28 controls. Data from 39 additional patients (22 PV and 17 BP) were now added. Eventually, we studied 67 patients (35 PV, 32 BP, 51 females), aged 64.7 ± 16.9 years and 67 age- gender- and body mass index-matched controls. In all subjects, serum 25OHVitD, calcium and alkaline phosphatase (ALP) levels were measured, bone mineral density (BMD) was evaluated by Dual-energy X-ray. Absorptiometry at lumbar spine (LS) and femoral neck (FN) and the presence of VFx were ascertained by visual assessment from spinal radiographs. In patients, the disease intensity was evaluated by the autoimmune bullous skin disorder intensity score (ABSIS).
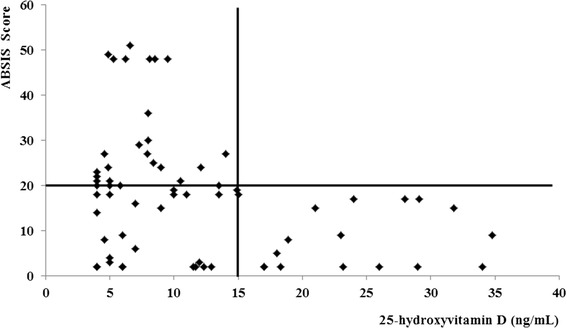
As compared with controls, both PV and BP patients showed lower 25OHVitD (22.2 ± 11.1 vs 13.9 ± 8.3 ng/mL, p < 0.001 and 22.4 ± 14.9 vs 9.5 ± 7.7 ng/mL, p < 0.0001, respectively) and higher prevalence of severe hypovitaminosis D (22.9 vs 48.6%, p < 0.02 and 31.1 vs 75.0%, p < 0.0001, respectively) and VFx (28.6 vs 57.1%, p = 0.03 and 34.4 vs 62.5%, P = 0.02, respectively). In both PV and BP patients, LS and FN BMD did not differ from controls. In the whole patients' group, ABSIS score was inversely associated with 25OHVitD levels (R = -0.36, p < 0.005), regardless of age (β = -3.2, P = 0.009).
PV and BP patients have an increased prevalence of hypovitaminosis D and VFx. The extended study shows, for the first time, that the 25OHVitD levels are inversely associated with disease intensity and that VFx occur in spite of a not reduced BMD.
自身免疫性大疱性皮肤病患者,如寻常型天疱疮(PV)和大疱性类天疱疮(BP),是否存在维生素D缺乏症仍存在争议。在之前的一项研究中,我们发现PV和BP患者椎骨骨折(VFx)和维生素D缺乏症的患病率增加。本研究扩大了前一项研究的样本量,以调查这些患者的25-羟基维生素D(25OHVitD)水平与骨骼健康和疾病严重程度的关系。
前一项研究纳入了13例PV患者、15例BP患者和28例对照。现在又增加了39例患者(22例PV和17例BP)的数据。最终,我们研究了67例患者(35例PV、32例BP、51例女性),年龄为64.7±16.9岁,并与67例年龄、性别和体重指数匹配的对照进行比较。所有受试者均检测血清25OHVitD、钙和碱性磷酸酶(ALP)水平,采用双能X线吸收法评估腰椎(LS)和股骨颈(FN)的骨密度(BMD),并通过脊柱X线片的视觉评估确定是否存在VFx。在患者中,通过自身免疫性大疱性皮肤病严重程度评分(ABSIS)评估疾病严重程度。
与对照组相比,PV和BP患者的25OHVitD水平均较低(分别为22.2±11.1 vs 13.9±8.3 ng/mL,p<0.001和22.4±14.9 vs 9.5±7.7 ng/mL,p<0.0001),严重维生素D缺乏症的患病率较高(分别为22.9% vs 48.6%,p<0.02和31.1% vs 75.0%,p<0.0001),VFx的患病率也较高(分别为28.6% vs 57.1%,p=0.03和34.4% vs 62.5%,P=0.02)。PV和BP患者的LS和FN BMD与对照组无差异。在整个患者组中,无论年龄如何,ABSIS评分与25OHVitD水平呈负相关(R=-0.36,p<0.005)(β=-3.2,P=0.009)。
PV和BP患者维生素D缺乏症和VFx的患病率增加。这项扩展研究首次表明,25OHVitD水平与疾病严重程度呈负相关,尽管BMD未降低,但仍会发生VFx。