Schuette Claudia, Steffens Daniel, Witkowski Marco, Stellbaum Caroline, Bobbert Peter, Schultheiss Heinz-Peter, Rauch Ursula
Department of Internal Medicine/Cardiology, Campus Benjamin Franklin, Charité - Universitätsmedizin Berlin, Hindenburgdamm 30, 12200, Berlin, Germany.
Cardiovasc Diabetol. 2015 Feb 3;14:15. doi: 10.1186/s12933-015-0182-7.
Although antiplatelet therapy involving clopidogrel is a standard treatment for preventing cardiovascular events after coronary stent implantation, patients can display differential responses. Here, we assessed the effectiveness of clopidogrel on platelet function inhibition in subjects with and without type-2 diabetes and stable coronary artery disease. In addition, we investigated the correlation between platelet function and routine clinical parameters.
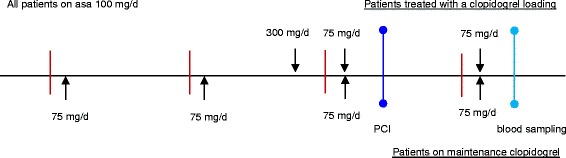
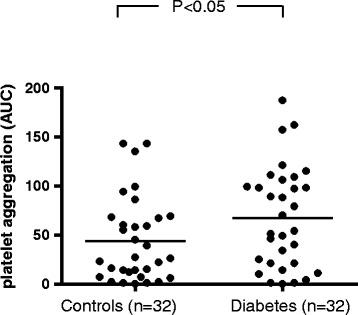
A total of 64 patients with stable coronary heart disease were enrolled in the study. Among these, 32 had known type-2 diabetes, whereas the remaining 32 subjects were non-diabetics (control group). A loading dose of 300 mg clopidogrel was given to clopidogrel-naïve patients (13 patients in the diabetes group and 14 control patients). All patients were given a daily maintenance dose of 75 mg clopidogrel. In addition, all patients received 100 mg ASA per day. Agonist-induced platelet aggregation measurements were performed on hirudin-anticoagulated blood using an impedance aggregometer (Multiple Platelet Function Analyzer, Dynabyte, Munich, Germany). Blood samples were drawn from the antecubital vein 24 h after coronary angiography with percutaneous coronary intervention. The platelets were then stimulated with ADP alone or ADP and prostaglandin-E (ADP and ADP-PGE tests, respectively) in order to evaluate clopidogrel-mediated inhibition of platelet function. The effectiveness of ASA was measured by stimulation with arachidonic acid (ASPI test). In addition, maximal platelet aggregation was assessed via stimulation with thrombin receptor-activating peptide (TRAP test).
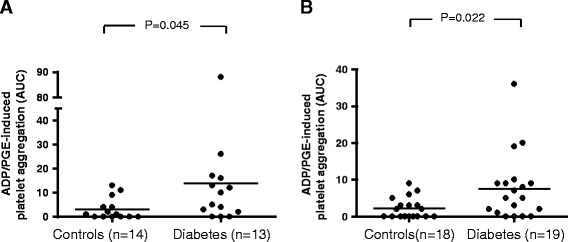
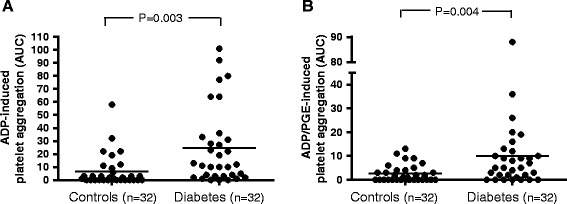
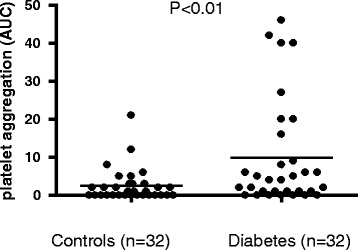
Patients with diabetes exhibited significantly less inhibition of platelet function than patients without diabetes (ADP-PGE test p = 0.003; ASPI test p = 0.022). Administering a clopidogrel loading dose of 300 mg did not result in a lower level of ADP-PGE-induced platelet reactivity in comparison to the use of a 75 mg maintenance dose. Moreover, we observed that ADP-PGE-induced platelet inhibition was positively correlated with fasting blood glucose and HbA1c (p < 0.01).
Patients with type-2 diabetes exhibited increased platelet reactivity compared to patients without diabetes despite combined treatment with clopidogrel and ASA. Using a loading dose of clopidogrel rather than small daily doses was not sufficient for adequately overcoming increased platelet reactivity in patients with type-2 diabetes, highlighting the need for more effective anti-platelet drugs for such patients.
尽管氯吡格雷抗血小板治疗是冠状动脉支架植入术后预防心血管事件的标准治疗方法,但患者的反应可能存在差异。在此,我们评估了氯吡格雷对2型糖尿病患者和非2型糖尿病稳定型冠状动脉疾病患者血小板功能抑制的有效性。此外,我们还研究了血小板功能与常规临床参数之间的相关性。
本研究共纳入64例稳定型冠心病患者。其中,32例已知患有2型糖尿病,其余32例为非糖尿病患者(对照组)。对未服用过氯吡格雷的患者(糖尿病组13例,对照组14例)给予300 mg氯吡格雷负荷剂量。所有患者均给予每日75 mg氯吡格雷维持剂量。此外,所有患者每天服用100 mg阿司匹林。使用阻抗聚集仪(德国慕尼黑Dynabyte公司的多功能血小板功能分析仪)对水蛭素抗凝的血液进行激动剂诱导的血小板聚集测量。在经皮冠状动脉介入治疗后的冠状动脉造影24小时后,从前臂静脉采集血样。然后分别用二磷酸腺苷(ADP)或ADP与前列腺素E(分别为ADP和ADP-PGE试验)刺激血小板,以评估氯吡格雷介导的血小板功能抑制。通过用花生四烯酸刺激(ASPI试验)来测量阿司匹林的有效性。此外,通过用凝血酶受体激活肽刺激(TRAP试验)来评估最大血小板聚集。
糖尿病患者的血小板功能抑制明显低于非糖尿病患者(ADP-PGE试验p = 0.003;ASPI试验p = 0.022)。与使用75 mg维持剂量相比,给予300 mg氯吡格雷负荷剂量并未导致ADP-PGE诱导的血小板反应性降低。此外,我们观察到ADP-PGE诱导的血小板抑制与空腹血糖和糖化血红蛋白呈正相关(p < 0.01)。
尽管联合使用氯吡格雷和阿司匹林治疗,但2型糖尿病患者的血小板反应性高于非糖尿病患者。使用氯吡格雷负荷剂量而非小剂量每日给药不足以充分克服2型糖尿病患者血小板反应性的增加,这突出表明此类患者需要更有效的抗血小板药物。