Bar-On Lynn, Molenaers Guy, Aertbeliën Erwin, Van Campenhout Anja, Feys Hilde, Nuttin Bart, Desloovere Kaat
KU Leuven Department of Rehabilitation Sciences, 3000 Leuven, Belgium ; Clinical Motion Analysis Laboratory, University Hospital Leuven, 3212 Pellenberg, Belgium.
Clinical Motion Analysis Laboratory, University Hospital Leuven, 3212 Pellenberg, Belgium ; KU Leuven Department of Development and Regeneration, 3000 Leuven, Belgium ; Department of Orthopedics, University Hospital Leuven, 3212 Pellenberg, Belgium.
Biomed Res Int. 2015;2015:317047. doi: 10.1155/2015/317047. Epub 2015 Jan 11.
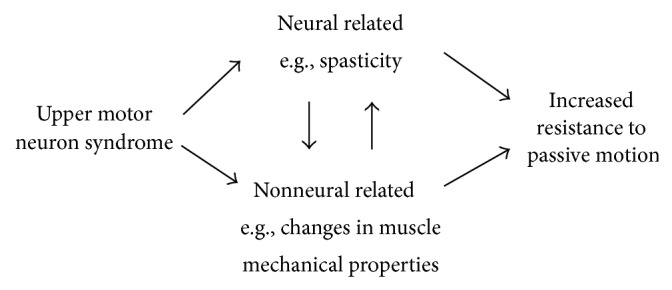
Spasticity is considered an important neural contributor to muscle hypertonia in children with cerebral palsy (CP). It is most often treated with antispasticity medication, such as Botulinum Toxin-A. However, treatment response is highly variable. Part of this variability may be due to the inability of clinical tests to differentiate between the neural (e.g., spasticity) and nonneural (e.g., soft tissue properties) contributions to hypertonia, leading to the terms "spasticity" and "hypertonia" often being used interchangeably. Recent advancements in instrumented spasticity assessments offer objective measurement methods for distinction and quantification of hypertonia components. These methods can be applied in clinical settings and their results used to fine-tune and improve treatment. We reviewed current advancements and new insights with respect to quantifying spasticity and its contribution to muscle hypertonia in children with CP. First, we revisit what is known about spasticity in children with CP, including the various definitions and its pathophysiology. Second, we summarize the state of the art on instrumented spasticity assessment in CP and review the parameters developed to quantify the neural and nonneural components of hypertonia. Lastly, the impact these quantitative parameters have on clinical decision-making is considered and recommendations for future clinical and research investigations are discussed.
痉挛被认为是导致脑瘫(CP)患儿肌肉张力亢进的一个重要神经因素。它最常使用抗痉挛药物进行治疗,如A型肉毒毒素。然而,治疗反应差异很大。这种差异的部分原因可能是临床测试无法区分导致张力亢进的神经因素(如痉挛)和非神经因素(如软组织特性),导致“痉挛”和“张力亢进”这两个术语经常互换使用。仪器化痉挛评估的最新进展提供了区分和量化张力亢进成分的客观测量方法。这些方法可应用于临床环境,其结果可用于微调并改善治疗。我们回顾了目前在量化痉挛及其对CP患儿肌肉张力亢进的影响方面的进展和新见解。首先,我们重新审视关于CP患儿痉挛的已知情况,包括各种定义及其病理生理学。其次,我们总结了CP患儿仪器化痉挛评估的现状,并回顾了为量化张力亢进的神经和非神经成分而开发的参数。最后,考虑了这些定量参数对临床决策的影响,并讨论了未来临床和研究调查的建议。