Saver Jeffrey L, Starkman Sidney, Eckstein Marc, Stratton Samuel J, Pratt Franklin D, Hamilton Scott, Conwit Robin, Liebeskind David S, Sung Gene, Kramer Ian, Moreau Gary, Goldweber Robert, Sanossian Nerses
From the Comprehensive Stroke Center (J.L.S., S.S., D.S.L.) and the Departments of Neurology (J.L.S., S.S., D.S.L.) and Emergency Medicine (S.S., F.P.), David Geffen School of Medicine at the University of California, Los Angeles (UCLA), the Departments of Emergency Medicine (M.E.) and Neurology (G.S., N.S.), Keck School of Medicine of the University of Southern California, the Los Angeles Fire Department (M.E.), the Los Angeles County Fire Department (F.P.), the Department of Emergency Medicine, Presbyterian Intercommunity Hospital (I.K.), the Department of Emergency Medicine, Long Beach Memorial Medical Center (G.M.), and the Department of Emergency Medicine, Huntington Memorial Hospital (R.G.), Los Angeles, the Los Angeles County Emergency Medical Services (EMS) Agency, the Orange County EMS Agency, and the Department of Emergency Medicine, Harbor-UCLA Medical Center, Torrance (S.J.S.), and Stanford University, Palo Alto (S.H.) - all in California; and the National Institute of Neurological Disorders and Stroke, Bethesda, MD (R.C.).
N Engl J Med. 2015 Feb 5;372(6):528-36. doi: 10.1056/NEJMoa1408827.
Magnesium sulfate is neuroprotective in preclinical models of stroke and has shown signals of potential efficacy with an acceptable safety profile when delivered early after stroke onset in humans. Delayed initiation of neuroprotective agents has hindered earlier phase 3 trials of neuroprotective agents.
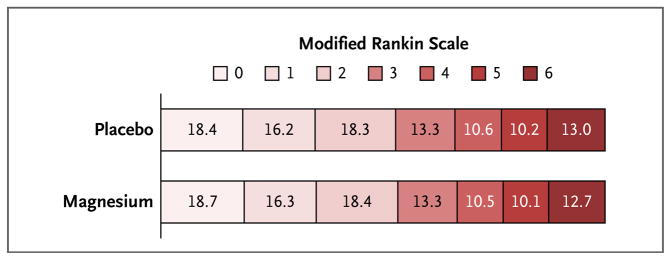
We randomly assigned patients with suspected stroke to receive either intravenous magnesium sulfate or placebo, beginning within 2 hours after symptom onset. A loading dose was initiated by paramedics before the patient arrived at the hospital, and a 24-hour maintenance infusion was started on the patient's arrival at the hospital. The primary outcome was the degree of disability at 90 days, as measured by scores on the modified Rankin scale (range, 0 to 6, with higher scores indicating greater disability).
Among the 1700 enrolled patients (857 in the magnesium group and 843 in the placebo group), the mean (±SD) age was 69±13 years, 42.6% were women, and the mean pretreatment score on the Los Angeles Motor Scale of stroke severity (range, 0 to 10, with higher scores indicating greater motor deficits) was 3.7±1.3. The final diagnosis of the qualifying event was cerebral ischemia in 73.3% of patients, intracranial hemorrhage in 22.8%, and a stroke-mimicking condition in 3.9%. The median interval between the time the patient was last known to be free of stroke symptoms and the start of the study-drug infusion was 45 minutes (interquartile range, 35 to 62), and 74.3% of patients received the study-drug infusion within the first hour after symptom onset. There was no significant shift in the distribution of 90-day disability outcomes on the global modified Rankin scale between patients in the magnesium group and those in the placebo group (P=0.28 by the Cochran-Mantel-Haenszel test); mean scores at 90 days did not differ between the magnesium group and the placebo group (2.7 in each group, P=1.00). No significant between-group differences were noted with respect to mortality (15.4% in the magnesium group and 15.5% in the placebo group, P=0.95) or all serious adverse events.
Prehospital initiation of magnesium sulfate therapy was safe and allowed the start of therapy within 2 hours after the onset of stroke symptoms, but it did not improve disability outcomes at 90 days. (Funded by the National Institute of Neurological Disorders and Stroke; FAST-MAG ClinicalTrials.gov number, NCT00059332.).
硫酸镁在中风临床前模型中具有神经保护作用,并且在人类中风发作后早期给药时显示出潜在疗效信号以及可接受的安全性。神经保护剂的延迟使用阻碍了神经保护剂早期的3期试验。
我们将疑似中风患者随机分配,在症状发作后2小时内开始接受静脉注射硫酸镁或安慰剂。在患者到达医院之前,急救人员先给予负荷剂量,患者到达医院后开始24小时维持输注。主要结局是90天时的残疾程度,采用改良Rankin量表评分(范围为0至6,分数越高表明残疾程度越高)进行测量。
在1700名入组患者中(硫酸镁组857例,安慰剂组843例),平均(±标准差)年龄为69±13岁,42.6%为女性,洛杉矶卒中严重程度运动量表(范围为0至10,分数越高表明运动功能缺损越严重)的平均治疗前评分为3.7±1.3。符合条件事件的最终诊断为脑缺血的患者占73.3%,颅内出血的患者占22.8%,类卒中情况的患者占3.9%。患者最后一次已知无中风症状到开始输注研究药物的中位间隔时间为45分钟(四分位间距为35至62分钟),74.3%的患者在症状发作后1小时内接受了研究药物输注。硫酸镁组和安慰剂组患者在全球改良Rankin量表上90天残疾结局分布无显著变化(Cochran-Mantel-Haenszel检验,P=0.28);硫酸镁组和安慰剂组90天时的平均评分无差异(每组均为2.7,P=1.00)。在死亡率(硫酸镁组为15.4%,安慰剂组为15.5%,P=0.95)或所有严重不良事件方面,未观察到显著的组间差异。
院前启动硫酸镁治疗是安全的,并能在中风症状发作后2小时内开始治疗,但并未改善90天时的残疾结局。(由美国国立神经疾病和中风研究所资助;FAST-MAG临床试验注册号,NCT00059332。)