Sacco Paul, Unick George Jay, Zanjani Faika, Camlin Elizabeth A S
a School of Social Work , University of Maryland , Baltimore , Maryland , USA.
J Dual Diagn. 2015;11(1):83-92. doi: 10.1080/15504263.2014.993295.
The prevalence of depression in older adults has been increasing over the last 20 years and is associated with economic costs in the form of treatment utilization and caregiving, including inpatient hospitalization. Comorbid alcohol diagnoses may serve as a complicating factor in inpatient admissions and may lead to overutilization of care and greater economic cost. This study sought to isolate the comorbidity effect of alcohol among older adult hospital admissions for depression.
We analyzed a subsample (N = 8,480) of older adults (65+) from the 2010 Nationwide Inpatient Sample who were hospitalized with primary depression diagnoses, 7,741 of whom had depression only and 739 of whom also had a comorbid alcohol disorder. To address potential selection bias based on drinking and health status, propensity score matching was used to compare length of stay, total costs, and disposition between the two groups.
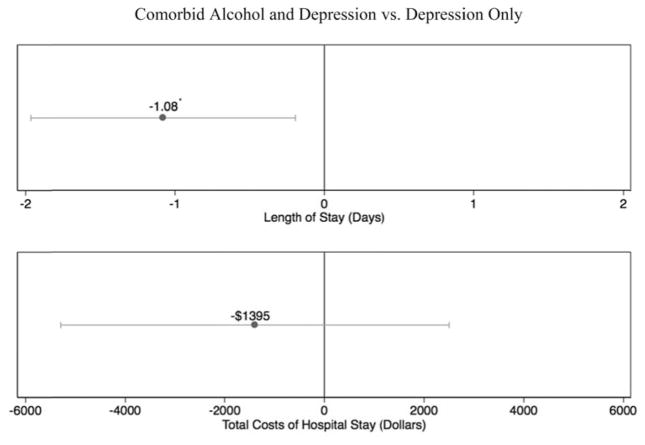
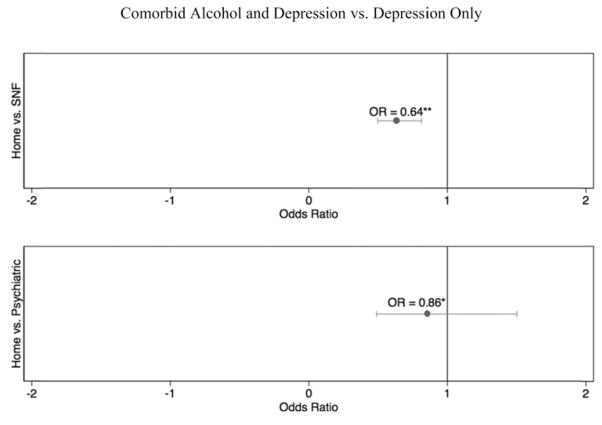
Bivariate analyses showed that older persons with depression and alcohol comorbidities were more often male (59.9% versus 34.0%, p <.001) and younger (70.9 versus 75.9 years, p <.001) than those with depression only. In terms of medical comorbidities, those with depression and alcohol disorders experienced more medical issues related to substance use (e.g., drug use diagnoses, liver disease, and suicidality; all p <.001), while those with depression only experienced more general medical problems (e.g., diabetes, renal failure, hypothyroid, and dementia; all p <.001). Propensity score matched models found that alcohol comorbidity was associated with shorter lengths of stay (on average 1.08 days, p <.02) and lower likelihood of post-hospitalization placement in a nursing home or other care facility (OR = 0.64, p <.001). No significant differences were found in overall costs or likelihood of discharge to a psychiatric hospital.
In older adults, depression with alcohol comorbidity does not lead to increased costs or higher levels of care after discharge. Comorbidity may lead to inpatient hospitalization at lower levels of severity, and depression with alcohol comorbidity may be qualitatively different than non-comorbid depression. Additionally, increased costs and negative outcomes in this population may occur at other levels of care such as outpatient services or emergency department visits.
在过去20年中,老年人抑郁症的患病率一直在上升,并且与治疗利用和护理(包括住院治疗)形式的经济成本相关。酒精共病诊断可能是住院治疗中的一个复杂因素,可能导致过度使用医疗服务并产生更高的经济成本。本研究旨在分离老年人因抑郁症住院时酒精共病的影响。
我们分析了2010年全国住院患者样本中65岁及以上老年人的一个子样本(N = 8480),这些患者因原发性抑郁症诊断而住院,其中7741人仅患有抑郁症,739人还患有酒精共病。为了解决基于饮酒和健康状况的潜在选择偏倚,采用倾向得分匹配法比较两组之间的住院时间、总费用和出院处置情况。
双变量分析显示,与仅患有抑郁症的老年人相比,患有抑郁症和酒精共病的老年人男性比例更高(59.9%对34.0%,p <.001)且年龄更小(70.9岁对75.9岁,p <.001)。在医疗共病方面,患有抑郁症和酒精障碍的老年人经历了更多与物质使用相关的医疗问题(如药物使用诊断、肝病和自杀倾向;所有p <.001),而仅患有抑郁症的老年人经历了更多的一般医疗问题(如糖尿病、肾衰竭、甲状腺功能减退和痴呆;所有p <.001)。倾向得分匹配模型发现,酒精共病与住院时间缩短(平均缩短1.08天,p <.02)以及出院后入住养老院或其他护理机构的可能性降低相关(OR = 0.64,p <.001)。在总费用或出院到精神病医院的可能性方面未发现显著差异。
在老年人中,抑郁症合并酒精共病并不会导致出院后费用增加或护理水平提高。共病可能导致病情较轻时住院治疗,并且抑郁症合并酒精共病在性质上可能与非共病抑郁症不同。此外,该人群在其他护理层面(如门诊服务或急诊就诊)可能会出现费用增加和不良后果。