Chang A H, Moisio K C, Chmiel J S, Eckstein F, Guermazi A, Prasad P V, Zhang Y, Almagor O, Belisle L, Hayes K, Sharma L
Department of Physical Therapy and Human Movement Sciences, Feinberg School of Medicine, Northwestern University, Chicago, IL, USA.
Department of Preventive Medicine, Feinberg School of Medicine, Northwestern University, Chicago, IL, USA.
Osteoarthritis Cartilage. 2015 Jul;23(7):1099-106. doi: 10.1016/j.joca.2015.02.005. Epub 2015 Feb 10.
Test the hypothesis that greater baseline peak external knee adduction moment (KAM), KAM impulse, and peak external knee flexion moment (KFM) during the stance phase of gait are associated with baseline-to-2-year medial tibiofemoral cartilage damage and bone marrow lesion progression, and cartilage thickness loss.
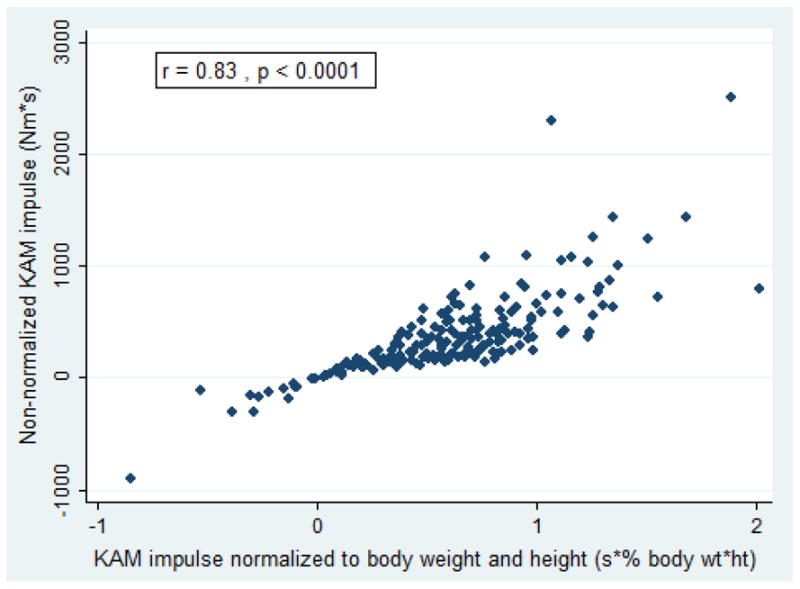
Participants all had knee OA in at least one knee. Baseline peak KAM, KAM impulse, and peak KFM (normalized to body weight and height) were captured and computed using a motion analysis system and six force plates. Participants underwent MRI of both knees at baseline and 2 years later. To assess the association between baseline moments and baseline-to-2-year semiquantitative cartilage damage and bone marrow lesion progression and quantitative cartilage thickness loss, we used logistic and linear regressions with generalized estimating equations (GEE), adjusting for gait speed, age, gender, disease severity, knee pain severity, and medication use.
The sample consisted of 391 knees (204 persons): mean age 64.2 years (SD 10.0); BMI 28.4 kg/m(2) (5.7); 156 (76.5%) women. Greater baseline peak KAM and KAM impulse were each associated with worsening of medial bone marrow lesions, but not cartilage damage. Higher baseline KAM impulse was associated with 2-year medial cartilage thickness loss assessed both as % loss and as a threshold of loss, whereas peak KAM was related only to % loss. There was no relationship between baseline peak KFM and any medial disease progression outcome measures.
Findings support targeting KAM parameters in an effort to delay medial OA disease progression.
验证以下假设,即步态站立期更大的基线膝关节外翻峰值内收力矩(KAM)、KAM冲量以及膝关节屈曲峰值力矩(KFM)与基线至2年的胫股内侧软骨损伤、骨髓病变进展以及软骨厚度丢失相关。
参与者至少一侧膝关节患有骨关节炎(OA)。使用运动分析系统和六个测力板采集并计算基线KAM峰值、KAM冲量以及KFM峰值(标准化为体重和身高)。参与者在基线时和2年后对双侧膝关节进行磁共振成像(MRI)检查。为评估基线力矩与基线至2年的半定量软骨损伤、骨髓病变进展以及定量软骨厚度丢失之间的关联,我们使用了广义估计方程(GEE)的逻辑回归和线性回归,并对步态速度、年龄、性别、疾病严重程度、膝关节疼痛严重程度以及药物使用情况进行了校正。
样本包括391个膝关节(204人):平均年龄64.2岁(标准差10.0);体重指数(BMI)28.4kg/m²(5.7);156名(76.5%)女性。更大的基线KAM峰值和KAM冲量均与内侧骨髓病变恶化相关,但与软骨损伤无关。更高的基线KAM冲量与2年内侧软骨厚度丢失相关,评估指标为丢失百分比和丢失阈值,而KAM峰值仅与丢失百分比相关。基线KFM峰值与任何内侧疾病进展结局指标之间均无关联。
研究结果支持将KAM参数作为延缓内侧OA疾病进展的目标。