Emory University, Atlanta, Georgia.
Arthritis Rheumatol. 2015 Mar;67(3):761-72. doi: 10.1002/art.38983.
To describe end-stage renal disease (ESRD) quality of care (receipt of pre-ESRD nephrology care, access to kidney transplantation, and placement of permanent vascular access for dialysis) in US patients with ESRD due to lupus nephritis (LN-ESRD) and to examine whether quality measures differ by patient sociodemographic characteristics or US region.
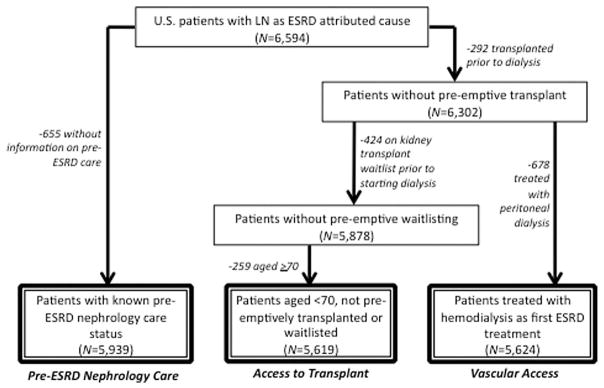
National surveillance data on patients in the US in whom treatment for LN-ESRD was initiated between July 2005 and September 2011 (n = 6,594) were analyzed. Odds ratios (ORs) and hazard ratios (HRs) with 95% confidence intervals (95% CIs) were determined for each quality measure, according to sociodemographic factors and US region.
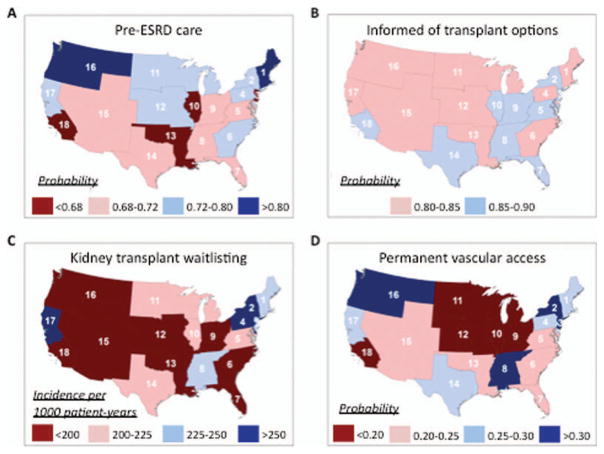
Overall, 71% of the patients received nephrology care prior to ESRD. Black and Hispanic patients were less likely than white patients to receive pre-ESRD care (OR 0.73 [95% CI 0.63-0.85] and OR 0.73 [95% CI 0.60-0.88], respectively) and to be placed on the kidney transplant waitlist within the first year after the start of ESRD (HR 0.78 [95% CI 0.68-0.91] and HR 0.82 [95% CI 0.68-0.98], respectively). Those with Medicaid (HR 0.51 [95% CI 0.44-0.58]) or no insurance (HR 0.36 [95% CI 0.29-0.44]) were less likely than those with private insurance to be placed on the waitlist. Only 24% had a permanent vascular access, and placement was even less likely among the uninsured (OR 0.62 [95% CI 0.49-0.79]). ESRD quality-of-care measures varied 2-3-fold across regions of the US, with patients in the Northeast and Northwest generally having higher probabilities of adequate care.
LN-ESRD patients have suboptimal ESRD care, particularly with regard to placement of dialysis vascular access. Minority race/ethnicity and lack of private insurance are associated with inadequate ESRD care. Further studies are warranted to examine multilevel barriers to, and develop targeted interventions to improve delivery of, care among patients with LN-ESRD.
描述美国狼疮性肾炎终末期肾病(ESRD)患者的 ESRD 质量护理(接受 ESRD 前肾病学护理、获得肾移植机会和进行透析用永久性血管通路置管),并探讨这些质量测量指标是否因患者社会人口统计学特征或美国地区而有所不同。
对 2005 年 7 月至 2011 年 9 月期间在美国开始接受狼疮性肾炎 ESRD 治疗的患者的全国监测数据进行分析(n=6594)。根据社会人口统计学因素和美国地区,确定每个质量测量指标的比值比(OR)和风险比(HR)及其 95%置信区间(95%CI)。
总体而言,71%的患者在 ESRD 之前接受了肾病学护理。与白人患者相比,黑人和西班牙裔患者接受 ESRD 前护理的可能性较低(OR 0.73[95%CI 0.63-0.85]和 OR 0.73[95%CI 0.60-0.88]),并且在 ESRD 开始后第一年被列入肾移植等待名单的可能性也较低(HR 0.78[95%CI 0.68-0.91]和 HR 0.82[95%CI 0.68-0.98])。那些拥有医疗补助(HR 0.51[95%CI 0.44-0.58])或没有保险(HR 0.36[95%CI 0.29-0.44])的患者比那些拥有私人保险的患者被列入等待名单的可能性更低。仅有 24%的患者有永久性血管通路,而没有保险的患者(OR 0.62[95%CI 0.49-0.79])的可能性更低。美国不同地区的 ESRD 质量护理指标差异为 2-3 倍,东北地区和西北地区的患者获得充足护理的概率通常更高。
狼疮性肾炎终末期肾病患者的 ESRD 护理不理想,特别是在进行透析血管通路置管方面。少数族裔和缺乏私人保险与 ESRD 护理不足有关。需要进一步研究,以检查影响患者接受护理的多层次障碍,并制定有针对性的干预措施,以改善狼疮性肾炎患者的护理。