TruneČka P, Klempnauer J, Bechstein W O, Pirenne J, Friman S, Zhao A, Isoniemi H, Rostaing L, Settmacher U, Mönch C, Brown M, Undre N, Tisone G
Transplantcentre, Institute for Clinical and Experimental Medicine, Prague, Czech Republic.
Department of General, Visceral and Transplantation Surgery, Hannover Medical School, Hannover, Germany.
Am J Transplant. 2015 Jul;15(7):1843-54. doi: 10.1111/ajt.13182. Epub 2015 Feb 23.
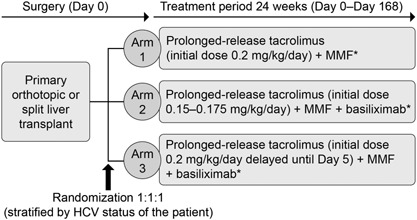
DIAMOND: multicenter, 24-week, randomized trial investigating the effect of different once-daily, prolonged-release tacrolimus dosing regimens on renal function after de novo liver transplantation. Arm 1: prolonged-release tacrolimus (initial dose 0.2mg/kg/day); Arm 2: prolonged-release tacrolimus (0.15-0.175mg/kg/day) plus basiliximab; Arm 3: prolonged-release tacrolimus (0.2mg/kg/day delayed until Day 5) plus basiliximab. All patients received MMF plus a bolus of corticosteroid (no maintenance steroids).
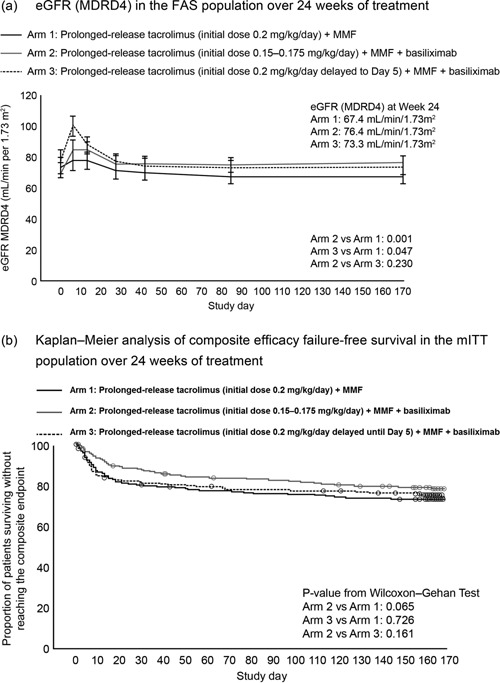
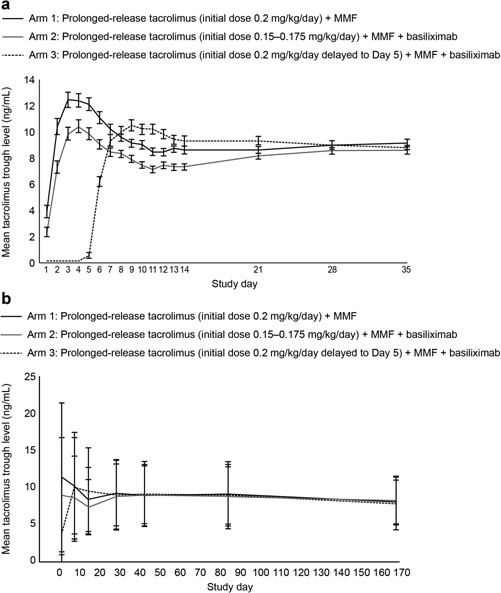
eGFR (MDRD4) at Week 24. Secondary endpoints: composite efficacy failure, BCAR and AEs. Baseline characteristics were comparable. Tacrolimus trough levels were readily achieved posttransplant; initially lower in Arm 2 versus 1 with delayed initiation in Arm 3. eGFR (MDRD4) was higher in Arms 2 and 3 versus 1 (p = 0.001, p = 0.047). Kaplan-Meier estimates of composite efficacy failure-free survival were 72.0%, 77.6%, 73.9% in Arms 1-3. BCAR incidence was significantly lower in Arm 2 versus 1 and 3 (p = 0.016, p = 0.039). AEs were comparable. Prolonged-release tacrolimus (0.15-0.175mg/kg/day) immediately posttransplant plus basiliximab and MMF (without maintenance corticosteroids) was associated with lower tacrolimus exposure, and significantly reduced renal function impairment and BCAR incidence versus prolonged-release tacrolimus (0.2mg/kg/day) administered immediately posttransplant. Delayed higher-dose prolonged-release tacrolimus initiation significantly reduced renal function impairment compared with immediate posttransplant administration, but BCAR incidence was comparable.
DIAMOND:一项多中心、为期24周的随机试验,研究不同的每日一次、缓释他克莫司给药方案对初次肝移植后肾功能的影响。第1组:缓释他克莫司(初始剂量0.2mg/kg/天);第2组:缓释他克莫司(0.15 - 0.175mg/kg/天)加巴利昔单抗;第3组:缓释他克莫司(0.2mg/kg/天延迟至第5天)加巴利昔单抗。所有患者均接受霉酚酸酯加一剂皮质类固醇(无维持性类固醇)。
第24周时的估算肾小球滤过率(MDRD4)。次要终点:综合疗效失败、活检证实的急性排斥反应(BCAR)和不良事件。基线特征具有可比性。移植后他克莫司谷浓度很容易达到;第2组最初低于第1组,第3组起始延迟。第2组和第3组的估算肾小球滤过率(MDRD4)高于第1组(p = 0.001,p = 0.047)。第1 - 3组的综合无疗效失败生存率的Kaplan - Meier估计值分别为72.0%、77.6%、73.9%。第2组的活检证实的急性排斥反应发生率显著低于第1组和第3组(p = 0.016,p = 0.039)。不良事件具有可比性。移植后立即给予缓释他克莫司(0.15 - 0.175mg/kg/天)加巴利昔单抗和霉酚酸酯(无维持性皮质类固醇)与较低的他克莫司暴露相关,与移植后立即给予缓释他克莫司(0.2mg/kg/天)相比,显著降低了肾功能损害和活检证实的急性排斥反应发生率。与移植后立即给药相比,延迟给予高剂量缓释他克莫司显著降低了肾功能损害,但活检证实的急性排斥反应发生率具有可比性。