Barriga-Rodríguez Paloma, Falcón-Cubillo Marta, Mejías-Trueba Marta, Ciudad-Gutiérrez Pablo, Guisado-Gil Ana Belén, Gómez-Bravo Miguel Ángel, Porras-López Manuel, Gil-Navarro María Victoria, Herrera-Hidalgo Laura
Department of Pharmacy, Virgen del Rocío University Hospital, 41013 Seville, Spain.
Institute of Biomedicine of Seville (IBiS), Virgen del Rocío University Hospital, Consejo Superior de Investigaciones Científicas (CSIC), University of Seville, 41013 Seville, Spain.
Pharmaceutics. 2025 May 6;17(5):619. doi: 10.3390/pharmaceutics17050619.
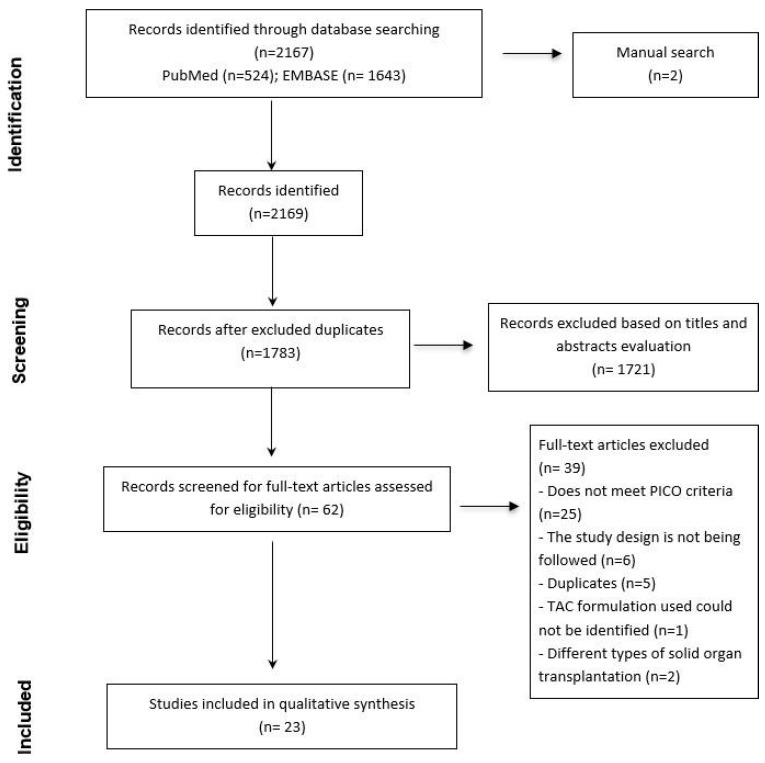
Tacrolimus (TAC) is the cornerstone of immunosuppression after liver transplantation (LT). TAC has a narrow therapeutic index and high inter- and intra-individual pharmacokinetic (PK) variability, requiring dose individualization. This variability is more noticeable in the early post-LT period. This study aimed to compare the PK of different TAC formulations in the early post-LT period and describe the main PK characteristics and plasma levels obtained with each TAC formulation used. The search was conducted in MEDLINE (PubMed) and EMBASE in accordance with PRISMA-ScR guidelines. The main inclusion criteria were clinical trials and observational studies focusing on the PK parameters of TAC in LT recipients during the first month post-transplant. A total of 2169 articles were identified, of which 23 met the inclusion criteria. Various PK parameters were analyzed after LT for the different TAC formulations: intravenous (iv) and oral forms, such as immediate-release (IRT), prolonged-release (PRT), and extended-release (LCPT) formulations. PK variability was higher in the initial days after LT, with different TAC exposure between formulations. IV TAC allows the rapid attainment of therapeutic levels, but it has fallen into disuse. Regarding oral formulations, IRT reaches target levels faster than PRT and LCPT. PRT and LCPT exposure seem more stable during the first month post-LT than when using IRT. TAC formulations exhibit relevant differences in their PK profile in the early post-LT period. PK differences might influence the dose regimen and the time to achieve PK targets. Given these variations, therapeutic drug monitoring (TDM) is essential for optimizing treatment.
他克莫司(TAC)是肝移植(LT)后免疫抑制的基石。TAC治疗指数窄,个体间和个体内药代动力学(PK)变异性高,需要个体化给药。这种变异性在LT术后早期更为明显。本研究旨在比较LT术后早期不同TAC制剂的PK,并描述每种TAC制剂的主要PK特征和血浆水平。检索按照PRISMA-ScR指南在MEDLINE(PubMed)和EMBASE中进行。主要纳入标准为关注LT受者移植后第一个月内TAC的PK参数的临床试验和观察性研究。共识别出2169篇文章,其中23篇符合纳入标准。对LT后不同TAC制剂的各种PK参数进行了分析:静脉注射(iv)和口服剂型,如速释(IRT)、缓释(PRT)和长效释放(LCPT)制剂。LT术后最初几天PK变异性较高,不同制剂之间TAC暴露情况不同。静脉注射TAC可快速达到治疗水平,但已不再使用。对于口服制剂,IRT比PRT和LCPT更快达到目标水平。在LT术后第一个月,PRT和LCPT的暴露似乎比使用IRT时更稳定。TAC制剂在LT术后早期的PK谱表现出相关差异。PK差异可能会影响给药方案和达到PK目标的时间。鉴于这些差异,治疗药物监测(TDM)对于优化治疗至关重要。