Tamaki Ichiro, Obama Kazutaka, Matsuo Koichi, Kami Kazuhiro, Uemoto Yusuke, Sato Teruyuki, Ito Tetsuo, Tamaki Nobuyuki, Kubota Keiko, Inoue Hidenobu, Yamamoto Eiji, Morimoto Taisuke
Kyoto City Hospital, Department of Surgery, Mibuhigashitakadacho 1-2, Nakagyo Ward, Kyoto City, Kyoto Pref., Japan.
Kyoto City Hospital, Department of Surgery, Mibuhigashitakadacho 1-2, Nakagyo Ward, Kyoto City, Kyoto Pref., Japan.
Int J Surg Case Rep. 2015;9:34-8. doi: 10.1016/j.ijscr.2015.02.031. Epub 2015 Feb 19.
We report a case of primary adenocarcinoma in the third portion of the duodenum (D3) curatively resected by laparoscopic and endoscopic cooperating surgery (LECS).
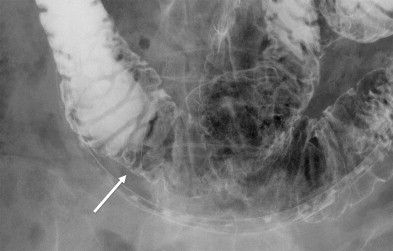
A 65-year-old woman had a routine visit to our hospital for a follow-up of rectal cancer resected curatively 2 years ago. A routine screening gastroduodenal endoscopy revealed an elevated lesion of 20mm in diameter in the D3. The preoperative diagnosis was adenoma with high-grade dysplasia; however, suspicion about potential adenocarcinoma was undeniable. Curative resection was performed by LECS. Pathological examination revealed intramucosal adenocarcinoma arising from normal duodenal mucosa. The tumor was stage I (T1/N0/M0) in terms of the tumor, nodes, metastasis (TNM) classification. LECS for duodenal tumor has seldom been reported previously, and this is the first report of LECS for primary adenocarcinoma in the D3. The transverse mesocolon was removed from the head of pancreas to expose the duodenum, and the accessory right colic vein was cut; this was followed by the Kocher maneuver for mobilization of the lesion site.
LECS enabled en bloc resection with adequate surgical margins and secure intra-abdominal suturing. Thorough mobilization of the mesocolon and pancreas head is essential for this procedure because it facilitates correct resection and suturing.
LECS is a feasible treatment option for duodenal neoplasms, including intramucosal adenocarcinoma, even though it exists in the D3.
我们报告一例通过腹腔镜与内镜合作手术(LECS)根治性切除十二指肠第三部分(D3)原发性腺癌的病例。
一名65岁女性因2年前根治性切除直肠癌来我院进行常规复诊。常规的胃十二指肠内镜检查发现D3处有一个直径20mm的隆起性病变。术前诊断为高级别异型增生腺瘤;然而,对潜在腺癌的怀疑是不可否认的。通过LECS进行了根治性切除。病理检查显示肿瘤起源于正常十二指肠黏膜的黏膜内腺癌。根据肿瘤、淋巴结、转移(TNM)分类,该肿瘤为I期(T1/N0/M0)。此前很少有关于十二指肠肿瘤LECS的报道,这是首例关于D3原发性腺癌LECS的报道。将横结肠系膜从胰头处分离以暴露十二指肠,并切断副右结肠静脉;随后进行 Kocher 手法以游离病变部位。
LECS能够实现整块切除并获得足够的手术切缘以及可靠的腹腔内缝合。对于该手术,彻底游离结肠系膜和胰头至关重要,因为这有助于正确的切除和缝合。
LECS是十二指肠肿瘤(包括黏膜内腺癌)的一种可行治疗选择,即使肿瘤位于D3。