Nakamura Masanao, Hirooka Yoshiki, Watanabe Osamu, Yamamura Takeshi, Furukawa Kazuhiro, Funasaka Kohei, Ohno Eizaburo, Miyahara Ryoji, Kawashima Hiroki, Ando Takafumi, Ohmiya Naoki, Goto Hidemi
Department of Gastroenterology and Hepatology, Nagoya University Graduate School of Medicine, Nagoya, Japan.
Department of Endoscopy, Nagoya University Hospital, Nagoya, Japan.
Nagoya J Med Sci. 2014 Aug;76(3-4):369-74.
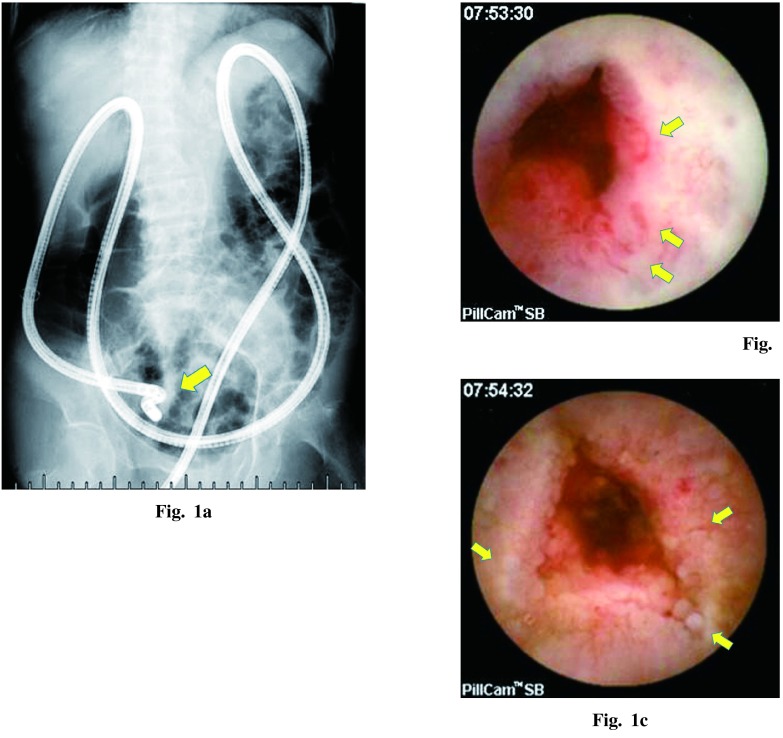
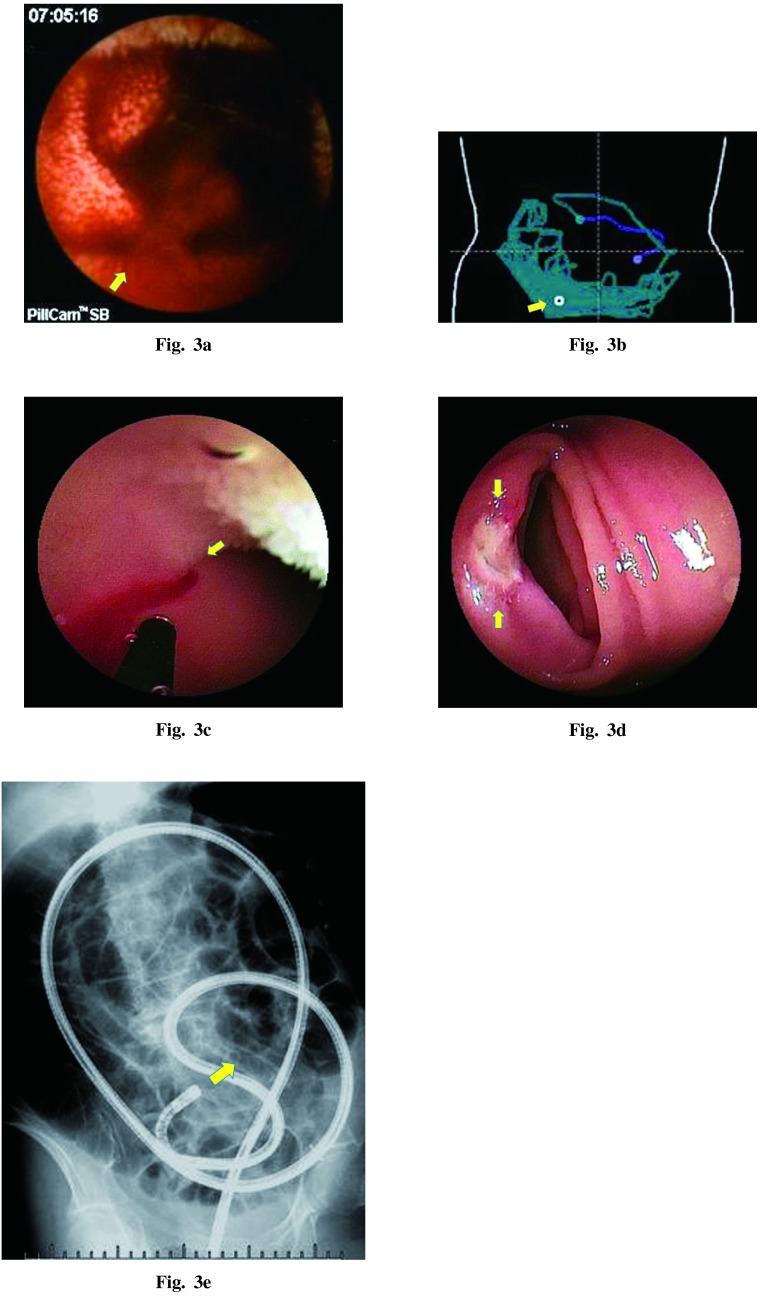
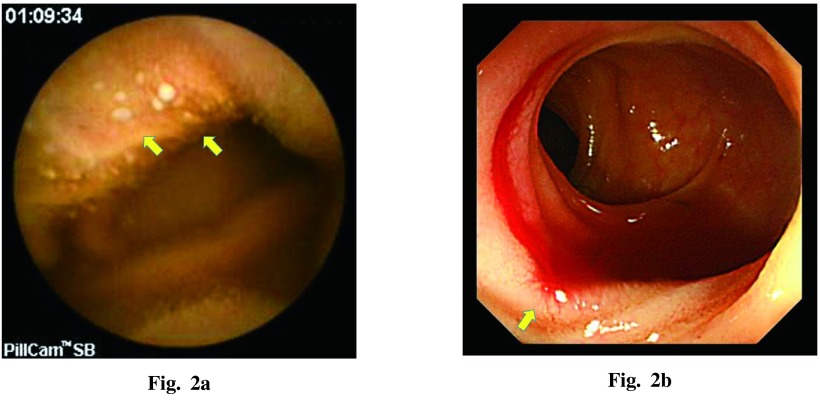
Endoscopic exploration of the small bowel after pelvic radiation has limitations related to strong abdominal adhesion. It is often difficult to demonstrate the findings of radiation enteritis endoscopically, even with video capsule endoscopy (VCE) or double-balloon enteroscopy (DBE). We present our experience with three cases of radiation enteritis that were diagnosed using VCE and DBE, including their effective aspects. Radiation enteritis has not been diagnosed using conventional methods, and DBE may not accomplish deeper insertion into the ileum, although it is capable of both diagnosis and hemostasis. Therefore, VCE is thought to be the initial tool for the diagnosis of radiation enteritis when small bowel stenosis has not been previously detected and the risk of retention has been discussed.
盆腔放疗后小肠的内镜检查因严重的腹部粘连而存在局限性。即使使用视频胶囊内镜(VCE)或双气囊小肠镜(DBE),通过内镜检查来证实放射性肠炎的表现也常常很困难。我们介绍三例使用VCE和DBE诊断放射性肠炎的病例经验,包括其有效之处。放射性肠炎尚未通过传统方法确诊,DBE虽然能够进行诊断和止血,但可能无法更深地插入回肠。因此,当先前未检测到小肠狭窄且已讨论过滞留风险时,VCE被认为是诊断放射性肠炎的初始工具。