Kloth J S L, Pagani A, Verboom M C, Malovini A, Napolitano C, Kruit W H J, Sleijfer S, Steeghs N, Zambelli A, Mathijssen R H J
Department of Medical Oncology, Erasmus MC Cancer Institute, PO Box 5201, 3075EA Rotterdam, The Netherlands.
Department of Medical Oncology, Fondazione S. Maugeri, Via Maugeri 10, 27100 Pavia, Italy.
Br J Cancer. 2015 Mar 17;112(6):1011-6. doi: 10.1038/bjc.2015.82.
Tyrosine kinase inhibitors (TKIs) are associated with prolongation of the QTc interval on the electrocardiogram (ECG). The QTc-interval prolongation increases the risk of life-threatening arrhythmias. However, studies evaluating the effects of TKIs on QTc intervals are limited and only consist of small patient numbers.
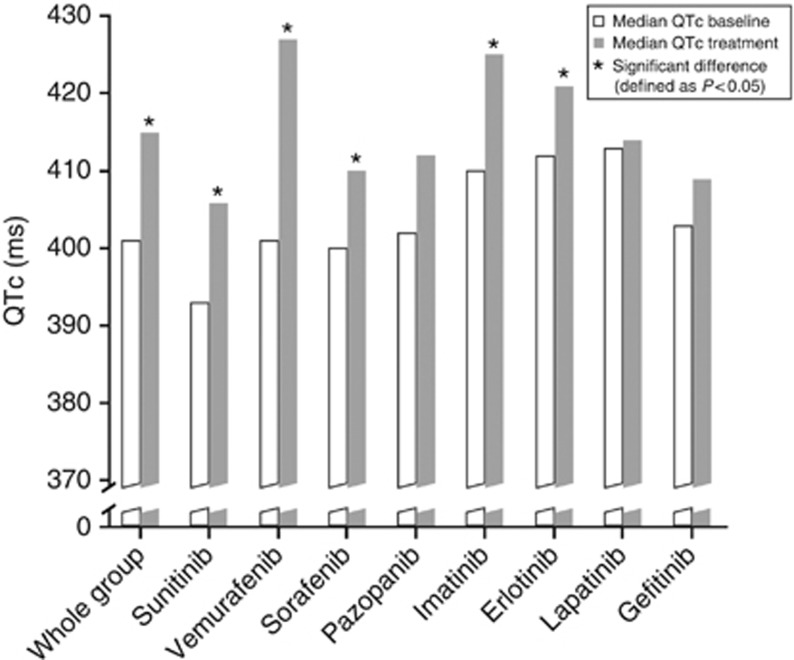
In this multicentre trial in four centres in the Netherlands and Italy we screened all patients who were treated with any TKI. To evaluate the effects of TKIs on the QTc interval, we investigated ECGs before and during treatment with erlotinib, gefitinib, imatinib, lapatinib, pazopanib, sorafenib, sunitinib, or vemurafenib.
A total of 363 patients were eligible for the analyses. At baseline measurement, QTc intervals were significantly longer in females than in males (QTcfemales=404 ms vs QTcmales=399 ms, P=0.027). A statistically significant increase was observed for the individual TKIs sunitinib, vemurafenib, sorafenib, imatinib, and erlotinib, after the start of treatment (median ΔQTc ranging from +7 to +24 ms, P<0.004). The CTCAE grade for QTc intervals significantly increased after start of treatment (P=0.0003). Especially patients who are treated with vemurafenib are at increased risk of developing a QTc of ⩾470 ms, a threshold associated with an increased risk for arrhythmias.
These observations show that most TKIs significantly increase the QTc interval. Particularly in vemurafenib-treated patients, the incidence of patients at risk for arrhythmias is increased. Therefore, especially in case of combined risk factors, ECG monitoring in patients treated with TKIs is strongly recommended.
酪氨酸激酶抑制剂(TKIs)与心电图(ECG)上QTc间期延长有关。QTc间期延长会增加危及生命的心律失常风险。然而,评估TKIs对QTc间期影响的研究有限,且样本量较小。
在荷兰和意大利四个中心开展的这项多中心试验中,我们筛查了所有接受任何TKI治疗的患者。为评估TKIs对QTc间期的影响,我们调查了使用厄洛替尼、吉非替尼、伊马替尼、拉帕替尼、帕唑帕尼、索拉非尼、舒尼替尼或维莫非尼治疗前及治疗期间的心电图。
共有363例患者符合分析条件。在基线测量时,女性的QTc间期显著长于男性(女性QTc = 404毫秒,男性QTc = 399毫秒,P = 0.027)。治疗开始后,舒尼替尼、维莫非尼、索拉非尼、伊马替尼和厄洛替尼等个别TKIs观察到有统计学意义的增加(QTc中位数变化范围为 +7至 +24毫秒,P < 0.004)。治疗开始后,QTc间期的CTCAE分级显著增加(P = 0.0003)。尤其是接受维莫非尼治疗的患者发生QTc≥470毫秒的风险增加,该阈值与心律失常风险增加相关。
这些观察结果表明,大多数TKIs会显著增加QTc间期。特别是在接受维莫非尼治疗的患者中,心律失常风险患者的发生率增加。因此,强烈建议对接受TKIs治疗的患者进行心电图监测,尤其是在存在合并危险因素的情况下。