Masenyetse Lieketseng J, Manda Samuel Om, Mwambi Henry G
Biostatistics Unit, South African Medical Research Council, Pretoria, South Africa ; School of Mathematics, Statistics and Computer Science, University of KwaZulu-Natal, Pietermaritzburg, South Africa.
School of Mathematics, Statistics and Computer Science, University of KwaZulu-Natal, Pietermaritzburg, South Africa.
AIDS Res Ther. 2015 Mar 5;12:6. doi: 10.1186/s12981-015-0044-0. eCollection 2015.
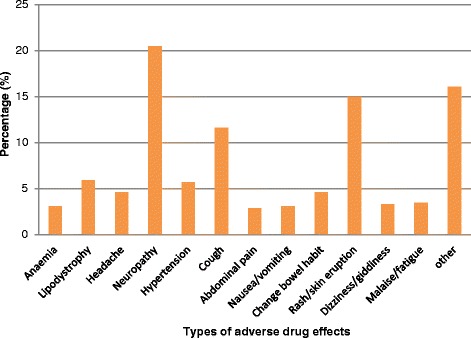
Antiretroviral treatment (ART) has been effective in reducing HIV/AIDS related morbidity and mortality. However, the use and uptake of ART has resulted in adverse reactions, due mainly to the medicine's toxicity and interactions with other medicines. The timing of adverse drug reactions (ADRs) among these patients is a critical public health issue for antiretroviral (ARV) treatment adherence and retention. Reliable monitoring of HIV patients on ART is through a structured pharmacovigilance surveillance system. However, recurrent nature of these data pose challenges in their analyses. This study aimed at modelling the timing of ADR events in HIV patients on ART using correlated time-to-event models.
The data concern 590 HIV patients registered onto the Medunsa National ARV Pharmacovigilance Surveillance System within 6 months of ART initiation between February 2007 and July 2011. Recurrent times of ADRs and baseline characteristics: patient gender, and age, ART regimen, clinic and initiation period were extracted from the data. The recurrent ADR events data were modelled using both shared frailty and marginal models on the five patients' characteristics as covariates.
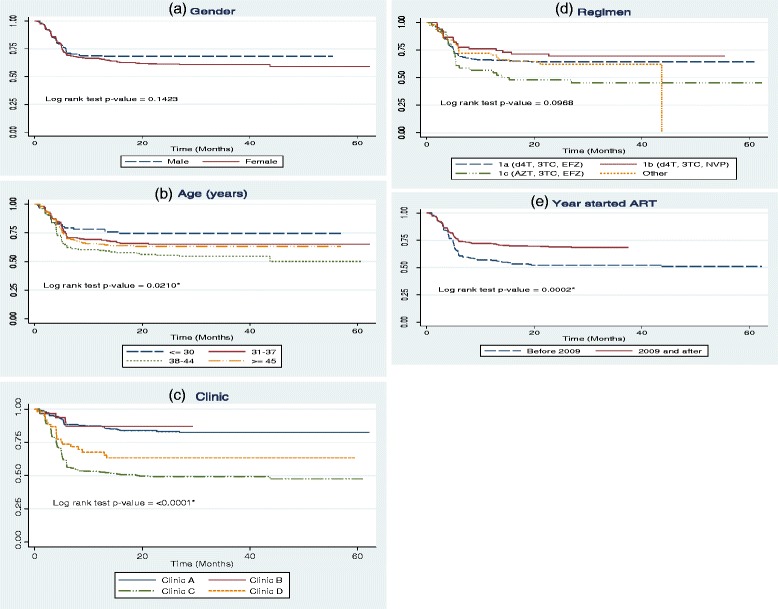
Out of 590 patients, 67% were female, 68% started on regimen: Stavudine, Lamivudine and Efavirenz; 37% had experienced at least one ADR and 67% started ART in 2009-2011. Age (p-value = 0.0210), clinic (p-value < 0.0001) and period of ART initiation (p-value = 0.0002) were significantly associated with timing of first ADR. There was a significantly higher rates of ADR recurrences in patients aged 38-44 years [HR = 2.45; 95% CI = (1.47; 4.10)] vs. 30 years and less, patients taking regimen: Zidovudine, Lamivudine and Nevarapine) vs. regimen: Stavudine, Lamivudine and Efavirenz [HR = 2.09; 95% CI = (1.35; 3.22)], while the rate was lower among those who started ART in 2009-2011 vs. those who initiated in 2007-2008 [HR = 0.55; 95% CI = (0.40; 0.76)].
More realistic time-to-event models for recurrent events data have been used to analyse timing of ADR events in HIV patients taking ARV treatment. Age, antiretroviral regimen type and period of initiation of ART were associated with the timing of HIV/AIDS drug related adverse reactions regardless of the analysis model used. This study has public health policy implications in addressing the added morbidity among HIV patients taking ARV treatment in the context of universal scaling up of ARV treatment.
抗逆转录病毒治疗(ART)在降低与艾滋病毒/艾滋病相关的发病率和死亡率方面已取得成效。然而,ART的使用引发了不良反应,主要是由于药物的毒性以及与其他药物的相互作用。这些患者中药物不良反应(ADR)的发生时间是抗逆转录病毒(ARV)治疗依从性和持续性的一个关键公共卫生问题。对接受ART的艾滋病毒患者进行可靠监测需通过结构化的药物警戒监测系统。然而,这些数据的重复性给分析带来了挑战。本研究旨在使用相关事件发生时间模型对接受ART的艾滋病毒患者ADR事件的发生时间进行建模。
数据涉及2007年2月至2011年7月期间在开始ART的6个月内登记到Medunsa国家ARV药物警戒监测系统的590名艾滋病毒患者。从数据中提取ADR的复发时间以及基线特征:患者性别、年龄、ART方案、诊所和开始治疗时间。将复发的ADR事件数据作为协变量,使用共享脆弱性模型和边际模型对患者的五个特征进行建模。
590名患者中,67%为女性,68%开始使用司他夫定、拉米夫定和依非韦伦方案;37%至少经历过一次ADR,67%在2009 - 2011年开始接受ART。年龄(p值 = 0.0210)、诊所(p值 < 0.0001)和ART开始时间(p值 = 0.0002)与首次ADR的发生时间显著相关。38 - 44岁患者的ADR复发率显著高于30岁及以下患者[风险比(HR)= 2.45;95%置信区间(CI)=(1.47;4.10)],使用齐多夫定、拉米夫定和奈韦拉平方案的患者与使用司他夫定、拉米夫定和依非韦伦方案的患者相比[HR = 2.09;95% CI =(1.35;3.22)],而2009 - 2011年开始接受ART的患者的复发率低于2007 - 2008年开始接受治疗的患者[HR = 0.55;95% CI =(0.40;0.76)]。
已使用更现实的针对复发事件数据的事件发生时间模型来分析接受ARV治疗的艾滋病毒患者ADR事件的发生时间。无论使用何种分析模型,年龄、抗逆转录病毒方案类型和ART开始时间均与艾滋病毒/艾滋病药物相关不良反应的发生时间有关。本研究在普遍扩大ARV治疗背景下解决接受ARV治疗的艾滋病毒患者额外发病率方面具有公共卫生政策意义。