Mansouri Alireza, Chan Vivien, Njaramba Veronica, Cadotte David W, Albright A Leland, Bernstein Mark
Division of Neurosurgery, Toronto Western Hospital, University Health Network, Hamilton, Canada ; Division of Neurosurgery, Department of Surgery, University of Toronto, Toronto, Hamilton, Canada ; Department of Clinical Epidemiology and Biostatistics, McMaster University, Hamilton, Canada.
Division of Neurosurgery, Toronto Western Hospital, University Health Network, Hamilton, Canada.
Surg Neurol Int. 2015 Feb 25;6:32. doi: 10.4103/2152-7806.152141. eCollection 2015.
Delay to neurosurgical care can result in significant morbidity and mortality. In this study, we aim to identify and quantify the sources of delay to neurosurgical consultation and care at a rural setting in Kenya.
A mixed-methods, cross-sectional analysis of all patients admitted to the neurosurgical department at Kijabe Hospital (KH) was conducted: A retrospective analysis of admissions from October 1 to December 31, 2013 and a prospective analysis from June 2 to June 20, 2014. Sources of delay were categorized and quantified. The Kruskal-Wallis test was used to identify an overall significant difference among diagnoses. The Mann-Whitney U test was used for pairwise comparisons within groups; the Bonferroni correction was applied to the alpha level of significance (0.05) according to the number of comparisons conducted. IBM SPSS version 22.0 (SPSS, Chicago, IL) was used for statistical analyses.
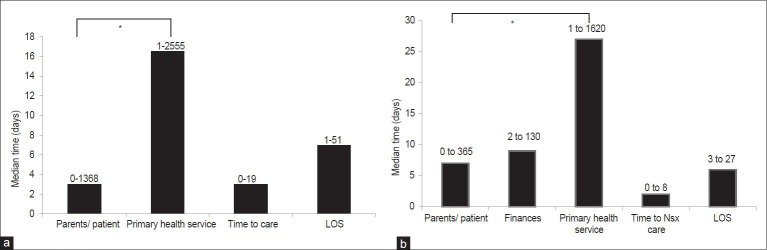
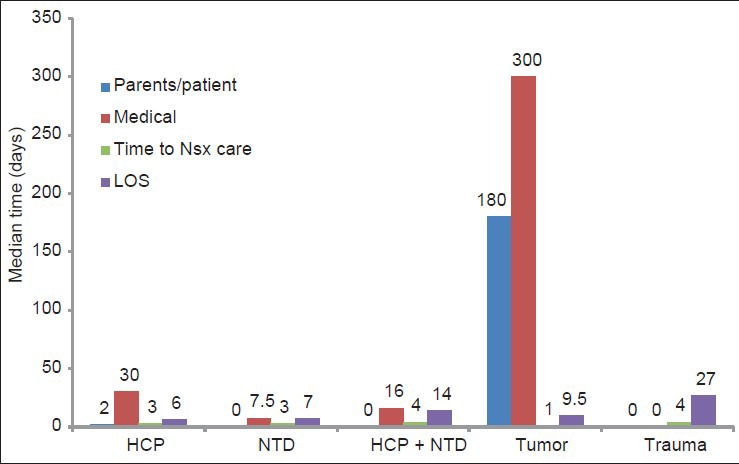
A total of 332 admissions were reviewed (237 retrospective, 95 prospective). The majority was pediatric admissions (median age: 3 months). Hydrocephalus (35%) and neural tube defects (NTDs; 27%) were most common. At least one source of delay was identified in 192 cases (58%); 39 (12%) were affected by multiple sources. Delay in primary care (PCPs), in isolation or combined with other sources, comprised 137 of total (71%); misdiagnosis or incorrect management comprised 46 (34%) of these. Finances contributed to delays in 25 of 95 prospective cases. At a median delay of 49 and 200.5 days, the diagnoses of hydrocephalus and tumors were associated with a significantly longer delay compared with NTDs (P < 0.001).
A substantial proportion of patients experienced delays in procuring pediatric neurosurgical care. Improvement in PCP knowledge base, implementation of a triage and referral process, and development of community-based funding strategies can potentially reduce these delays.
神经外科治疗的延迟会导致显著的发病率和死亡率。在本研究中,我们旨在确定并量化肯尼亚农村地区神经外科会诊及治疗延迟的来源。
对基贾贝医院(KH)神经外科收治的所有患者进行了混合方法的横断面分析:回顾性分析2013年10月1日至12月31日的入院病例,前瞻性分析2014年6月2日至6月20日的入院病例。对延迟来源进行分类和量化。采用Kruskal-Wallis检验确定不同诊断之间是否存在总体显著差异。采用Mann-Whitney U检验进行组内两两比较;根据进行比较的次数,将显著性水平α(0.05)进行Bonferroni校正。使用IBM SPSS 22.0版(SPSS,伊利诺伊州芝加哥)进行统计分析。
共审查了332例入院病例(回顾性237例,前瞻性95例)。大多数为儿科入院病例(中位年龄:3个月)。脑积水(35%)和神经管缺陷(NTDs;27%)最为常见。192例(58%)患者至少存在一个延迟来源;39例(12%)受多种来源影响。初级保健(PCP)的延迟,单独或与其他来源共同导致的延迟,占总数的137例(71%);其中误诊或错误管理占46例(34%)。在95例前瞻性病例中,25例的延迟与经济因素有关。脑积水和肿瘤诊断的中位延迟分别为49天和200.5天,与NTDs相比,延迟显著更长(P < 0.001)。
相当一部分患者在获得儿科神经外科治疗方面存在延迟。提高初级保健医生的知识水平、实施分诊和转诊流程以及制定基于社区的筹资策略可能会减少这些延迟。