Xourafas Dimitrios, Tavakkoli Ali, Clancy Thomas E, Ashley Stanley W
Harvard School of Public Health, Boston, MA, USA,
J Gastrointest Surg. 2015 May;19(5):831-40. doi: 10.1007/s11605-015-2788-1. Epub 2015 Mar 11.
The latest studies on surgical and cost-analysis outcomes after laparoscopic distal pancreatectomy (LDP) highlight mixed and insufficient results. Whereas several investigators have compared surgical outcomes of LDP vs. open distal pancreatectomy (ODP) for adenocarcinomas, few similar studies have focused on pancreatic neuroendocrine tumors (PNETs).
We reviewed the medical records of PNET patients undergoing distal pancreatectomy between 2004 and 2014. Patients were divided into LDP vs. ODP groups. Demographics, relevant comorbidities, oncologic variables, and cost-analysis data were assessed. Survival and Cox proportional hazards analyses were used to evaluate outcomes.
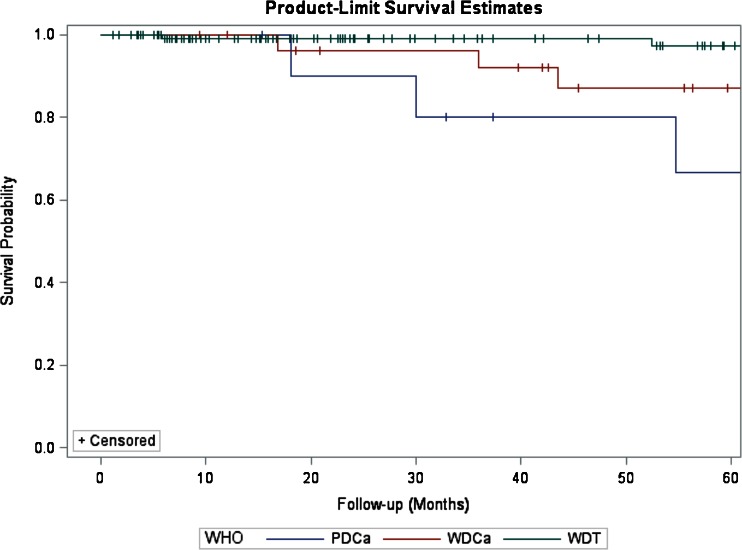
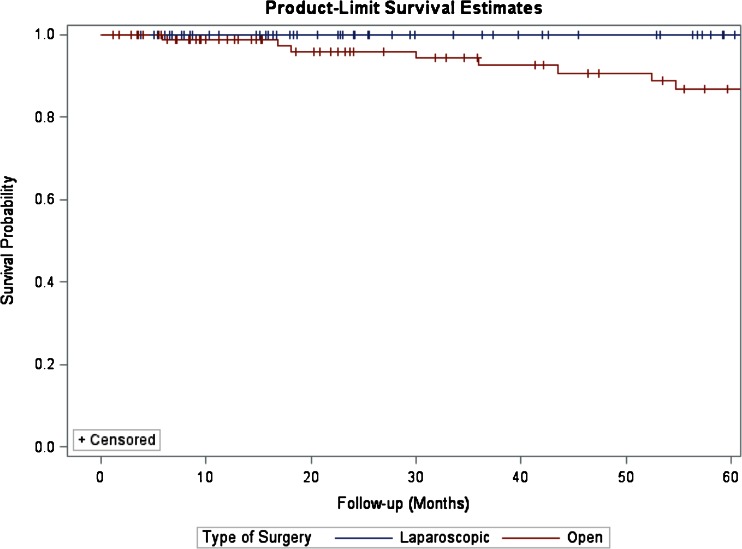
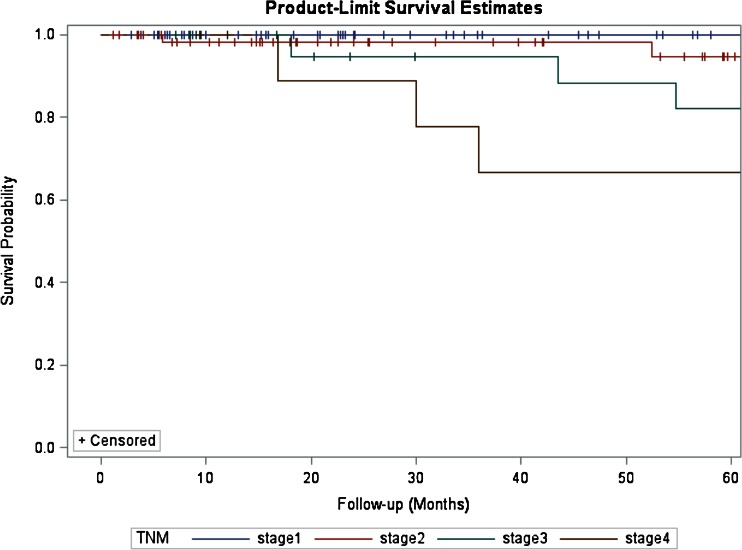
Of the 171 distal pancreatectomies for PNETs, 73 were laparoscopic, whereas 98 were open. Patients undergoing LDP demonstrated significantly lower rates of postoperative complications (P=0.028) and had significantly shorter hospital stays (P=0.008). On multivariable analysis, positive resection margins (P=0.046), G3 grade (P=0.036), advanced WHO classification (P=0.016), TNM stage (P=0.018), and readmission (P=0.019) were significantly associated with poor survival; however, method of resection (LDP vs. ODP) was not (P=0.254). The median total direct costs of LDP vs. ODP did not differ significantly.
In response to the recent considerable controversy surrounding the costs and surgical outcomes of LDP vs. ODP, our results show that LDP for PNETs is cost-neutral and significantly reduces postoperative morbidity without compromising oncologic outcomes and survival.
关于腹腔镜胰体尾切除术(LDP)术后的手术及成本分析结果的最新研究显示结果参差不齐且不充分。虽然有几位研究者比较了LDP与开放性胰体尾切除术(ODP)治疗腺癌的手术效果,但很少有类似研究关注胰腺神经内分泌肿瘤(PNETs)。
我们回顾了2004年至2014年间接受胰体尾切除术的PNET患者的病历。患者被分为LDP组和ODP组。评估了人口统计学、相关合并症、肿瘤学变量及成本分析数据。采用生存分析和Cox比例风险分析来评估预后。
在171例接受胰体尾切除术的PNET患者中,73例为腹腔镜手术,98例为开放手术。接受LDP的患者术后并发症发生率显著较低(P = 0.028),住院时间显著较短(P = 0.008)。多变量分析显示,切缘阳性(P = 0.046)、G3级(P = 0.036)、世界卫生组织高级别分类(P = 0.016)、TNM分期(P = 0.018)和再次入院(P = 0.019)与生存不良显著相关;然而,手术方式(LDP与ODP)与生存不良无关(P = 0.254)。LDP与ODP的总直接成本中位数无显著差异。
针对近期围绕LDP与ODP的成本及手术效果的大量争议,我们的结果表明,PNETs的LDP在成本方面无差异,且在不影响肿瘤学结局和生存的情况下显著降低了术后发病率。